
For more than 25 years, humans have lived and worked continuously aboard the International Space Station, conducting research that is transforming life on Earth and shaping the future of exploration. From growing food and sequencing DNA to…
Author: admin
-

Sci-Fi Cloaking Technology Takes a Step Closer to Reality With Synthetic Skin Like an Octopus
An octopus’s adaptive camouflage has long inspired materials scientists looking to come up with new cloaking technologies. Now researchers have created a synthetic “skin” that independently shifts its surface patterns and colors like these…
Continue Reading
-
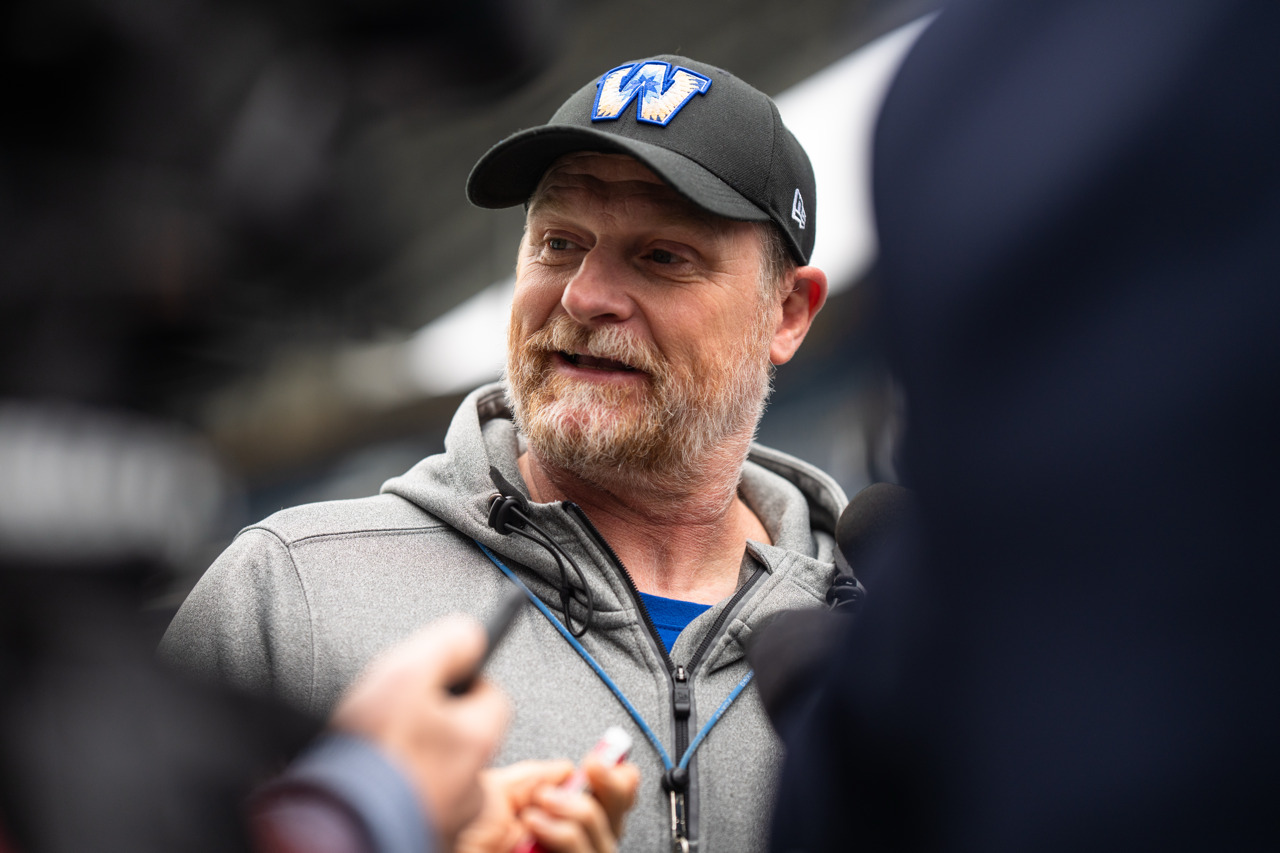
Notes from O’Shea/Walters and the CFL Winter Meetings
The Winnipeg Blue Bombers took some hefty swings in Canadian Football League free agency a year ago and will be wielding a heavy bat when the market opens in less than a month.
And while the organization has…
Continue Reading
-

Wildcats Debut at No. 24 in D1Baseball Rankings
TUCSON, Ariz. – The Arizona baseball team will commence the 2026 campaign ranked No. 24 in the nation in…
Continue Reading
-
Red Carpet Premiere of Bands of Enchantment Season 5 Celebrates City’s Creative Energy — City of Albuquerque
Tickets are now available for the red carpet premiere of the Emmy-winning music television series Bands of Enchantment: Albuquerque Sessions. Presented by Elkhorn Entertainment, in partnership with the City of Albuquerque’s Department of Arts &…
Continue Reading
-

The new Iranian revolution has begun
After a year that delivered crushing reversals to its regional sway and deterrence, Iran’s Islamic Republic has begun 2026 besieged by historic internal upheaval. The anti-government demonstrations that began percolating across the…
Continue Reading
-

Danny Freund Returns to North Dakota as Offensive Coordinator/Quarterbacks Coach
GRAND FORKS, N.D. – University of North Dakota head football coach Eric Schmidt announced the return of Danny Freund as the Fighting…
Continue Reading
-

Brolga Theatre records biggest year in 25 years
Published on 13 January 2026
A record-breaking 74,509 patrons attended performances and events at the Brolga Theatre and Convention Centre in 2025, the highest attendance in the venue’s 25-year history -…
Continue Reading
-

JCP gives go-ahead to three permanent IHC judges
ISLAMABAD:The Judicial Commission of Pakistan (JCP) has approved by…
Continue Reading
