- Yen Mostly Strengthens Amid Lingering Risks of Japan FX Intervention The Wall Street Journal
- Japanese Yen Forecast: BOJ Intervention, Election and Fed Speculation to Drive USD/JPY FOREX.com
- FX Daily Snapshot MUFG Research
- 6J: The Yen’s Make-or-Break Moment: Key Levels Every Trader Should Watch Barchart.com
- Yen strengthens after Japan warns of possible intervention TradingView — Track All Markets
Category: 3. Business
-
Yen Mostly Strengthens Amid Lingering Risks of Japan FX Intervention – The Wall Street Journal
-
Elliott Opposes Toyota Fudosan’s Revised Tender Offer for Toyota Industries Corporation
In the letter, Elliott outlined its opposition to the revised tender offer by Toyota Fudosan Co., Ltd. at ¥18,800 per share (the “Revised TOB”), which Elliott believes very significantly undervalues Toyota Industries. Elliott’s analysis showed the Company’s intrinsic net asset value to be more than ¥26,000 per share as of January 16, 2026 – almost 40% above the Revised TOB price – and that the Standalone Plan for Toyota Industries offers a clear path to a valuation of more than ¥40,000 per share by 2028.
The letter highlighted significant deficiencies in the transaction governance process and noted that if the Revised TOB succeeds, it would represent a setback for Japan’s corporate governance reforms and dampen investor interest in the Japanese market. Elliott does not intend to tender its shares into the Revised TOB and strongly encourages other shareholders not to tender.
The full text of the letter can be read at https://elliottletters.com and is included below:
Dear Fellow Shareholders of Toyota Industries Corporation:
We write on behalf of funds advised by Elliott Investment Management L.P. and Elliott Advisors (UK) Limited (together “Elliott” or “we”) as the largest minority investor in Toyota Industries Corporation (the “Company” or “Toyota Industries”).1 Our investment reflects our strong conviction in the Company, its value and its immense potential as a standalone business.
Based on our conversations with many of you, we know that you share our concerns regarding the attempt by Toyota Fudosan Co., Ltd (“Toyota Fudosan”) to squeeze out minority shareholders of Toyota Industries at a deeply discounted and unfair valuation in a coercive transaction. Although Toyota Fudosan’s revised tender offer bid at ¥18,800 per share (the “Revised TOB”) acknowledges the inadequacy of the original transaction terms, the new price continues to very substantially undervalue Toyota Industries, whose intrinsic net asset value is ¥26,134 per share or almost 40% above the Revised TOB price. If successful, the Revised TOB would represent a major setback for corporate governance, minority shareholder rights and fair M&A in Japan. Elliott opposes the Revised TOB as it is not in the best interests of minority shareholders and because we believe substantially more value can be generated by pursuing the Standalone Plan for the Company (described below) than by tendering into this wholly inadequate offer.
Elliott does not intend to tender its shares into the Revised TOB and we strongly encourage other shareholders not to tender.
Key Takeaways
Elliott has followed Toyota Industries for many years and has invested significant time and resources in underwriting its investment in the Company. We have worked with leading commercial consulting firms, former employees, industry executives, asset valuation experts, tax advisors, law firms and accountants to form our views on the Company’s business and significant financial assets.
Our conclusions are as follows:
- Toyota Industries owns world-class, market-leading businesses that are dominant in their respective areas, are exposed to positive secular tailwinds and have tremendous growth potential. These include the Company’s materials handling business, which is a global market leader and well positioned for future growth;
- Beyond its best-in-class operating businesses, Toyota Industries holds valuable minority stakes in publicly traded companies that together are worth more than the entire market capitalization at the Revised TOB price and account for two-thirds of the intrinsic net asset value (“NAV”) of Toyota Industries;
- The initial tender offer bid pre-announced on June 3, 2025 (the “Original TOB”) significantly undervalued Toyota Industries at ¥16,300 per share;
- Since the Original TOB was pre-announced, the value of Toyota Industries’ stakes in publicly traded companies has increased by more than 40% and its closest operating peer has appreciated by over 50% – yet the Revised TOB captures only a fraction of this increase, widening the gap to fair value;
- The transaction governance process remains deeply flawed, with deficiencies in the Original TOB only superficially addressed in the Revised TOB, representing a setback for corporate governance reform in Japan; and
- The Standalone Plan (described below) offers a clear path to NAV of more than ¥40,000 per share by 2028 – more than double the Revised TOB price.
A Fork in the Road for Toyota Industries Shareholders
The Revised TOB presents Toyota Industries shareholders with a choice that will determine the future of the Company. It is also a test of the effectiveness and credibility of Japanese corporate governance more broadly.
For more than a decade, Japanese policymakers, regulators and market participants have worked to improve the governance standards of the country’s world-class businesses and capital markets. The METI Fair M&A Guidelines2, the Guidelines for Corporate Takeovers3, the Code of Corporate Conduct in the Securities Listing Regulation4, and the broader effort to promote fair M&A practices are meant to protect shareholders in situations precisely like this one. The question now is whether those protections have substance – or whether, when tested, powerful companies like Toyota Industries can forcibly squeeze out their minority shareholders at a fraction of the investment’s fair value.
If a transaction on these terms is permitted to proceed – at a price representing a significant discount to fair value, through a process with structural conflicts, and over the objections of a broad coalition of institutional shareholders – it will send a discouraging signal about the effectiveness of Japan’s vital governance reforms and set a dangerous precedent for shareholders in other Japanese companies. The credibility of the Toyota Group and Japan’s capital markets are at stake. If, on the other hand, shareholders reject an inadequate offer and the Company pursues a path that maximizes value for all stakeholders, it will demonstrate that Japan’s governance modernization is real.
We believe this is a decisive moment. As the largest non-conflicted minority investor in Toyota Industries, we face a clear choice: accept an inadequate price, or decline to tender and retain ownership in a world-class industrial and materials handling business capable of delivering substantially greater value. Elliott is committed to the latter – and we believe it represents the better outcome for long-term shareholder value.
Significant Undervaluation from the Start
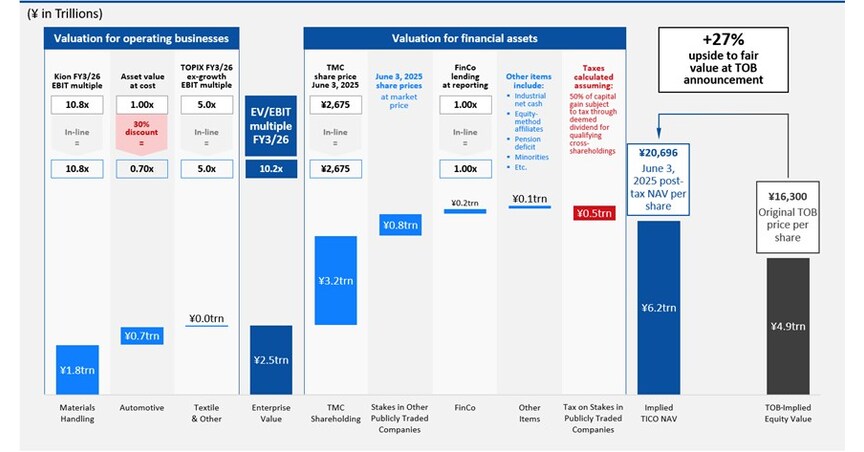
When the Original TOB at ¥16,300 per share was pre-announced on June 3, 2025, our valuation analysis showed Toyota Industries’ NAV to be ¥20,696 per share (see Appendix 1). Due to the Company’s opaque disclosures, we were not able to reconcile the significant gap between the Original TOB price and the Company’s true intrinsic value, but we suspect the key factors were some combination of:
- A discount applied to Toyota Industries’ stakes in publicly traded companies, which have a visible and known price and therefore cannot plausibly be undervalued in any offer;
- An inappropriately low valuation of the Company’s best-in-class operating businesses, including the world’s leading materials handling business; and
- No value given to the substantial tax savings available when unwinding cross-shareholdings through issuer buybacks. This structure benefits from a favorable deemed dividend treatment that Toyota Industries can utilize – and which it indeed envisages will be utilized, as part of both the Original and Revised TOB plans.
There was overwhelming consensus among market participants that the Original TOB was, at the time, fundamentally undervaluing Toyota Industries – evidenced by the share price trading 13% above the Original TOB price on the trading day before the pre-announcement. In our assessment, Toyota Industries’ NAV on June 3, 2025 – before any of the subsequent appreciation – was ¥20,696 per share, representing a 27% premium to the Original TOB price and a 10% premium to the Revised TOB price.
The Undervaluation Has Only Widened
Since the Original TOB was pre-announced, Toyota Industries’ intrinsic value has materially increased. Our analysis shows NAV of ¥26,134 per share on January 16, 2026 (see Appendix 2). Toyota Industries’ NAV has risen by ¥5,438 per share since the Original TOB, while the Revised TOB represents an increase of only ¥2,500 per share (see Appendix 3).
The key drivers of the demonstrable increase in NAV from June 3, 2025 to January 16, 2026 include:
- An increase in the value of Toyota Industries’ stakes in publicly traded companies. These stakes have increased in value by more than 40%, or ¥5,720 per share before tax. Net of tax, the value of these stakes has increased by ¥4,805 per share since the Original TOB was pre-announced; 5
- An increase in the market valuation of Toyota Industries’ core operating businesses. KION Group AG (“Kion”) is the most relevant peer company, given its number-two position in the global materials handling market. Kion’s share price increased by more than 50% between the Original TOB and the Revised TOB; and
- Cash generation by Toyota Industries, as well as other changes in assets and liabilities at the Company during this time period as customary in a NAV analysis, net of the settlement of the emissions-related class action lawsuit in the U.S.
In this context, the Revised TOB is wholly inadequate. The significant undervaluation evident at the time of the Original TOB pre-announcement on June 3, 2025 has not been addressed, nor will minority shareholders participate in the indisputable increase in the value of Toyota Industries’ stakes in publicly traded companies or in the market value of the Company’s operating businesses since the Original TOB.
The disconnect is evident from the final negotiations over the Revised TOB:
- On January 9, 2026, in response to a proposed offer price of ¥18,600, it was deemed that the price “still significantly deviates from the price level envisioned by the Company’s board of directors and the Special Committee, and must be largely increased also from the perspective of securing minority shareholders…in light of the fact that there is an increasing trend in the share prices of TMC and the Three Toyota Group Companies owned by the Company, the Tender Offer Price must be proposed factoring in the risk of price fluctuations up to the scheduled announcement date of commencement of the Tender Offer…”.6
- The Special Committee urged Toyota Fudosan to “substantially increase” the proposed offer price accordingly, acknowledging both the inadequacy of ¥18,600 and the rising value of the Company’s stakes in publicly traded companies.
- On January 12, 2026, Toyota Industries received the final Revised TOB price of ¥18,800 per share from Toyota Fudosan. On January 13, 2026, just one day after the proposal was received, Toyota Motor Corporation’s share price rose by 7.5% and the Company’s other stakes in publicly traded companies also increased in value. This rise resulted in a ¥1,005 per share increase in the post-tax intrinsic value of Toyota Industries – an increase which should have been fully accounted for in a further revised TOB price, but which was not.
- Despite the foregoing, on January 14, 2026, the Company accepted and recommended the Revised TOB price of ¥18,800 – just a cosmetic ¥200 more than the price which, days before, the Company had said deviated significantly from its expectations and needed to be substantially increased to safeguard minority shareholder interests – even before the increase in value of the Company’s stakes in publicly traded companies on January 13, 2026.
This example demonstrates that intrinsic value growth from Toyota Industries’ stakes in publicly traded companies has not been appropriately captured in the price negotiation process. It is therefore unsurprising that Toyota Industries’ representatives, at the January 14, 2026 press conference, were unable to explain how the significant increase in the value of the Company’s publicly traded stakes since the Original TOB announcement had been reflected in the Revised TOB price.
The deficiencies in the Revised TOB price are also evident from the shockingly low implied valuation under other methodologies:
- Less than 1x estimated book value: The Revised TOB price is materially below our estimate of IFRS book value as of December 31, 2025 (see Appendix 4). It is even further below our pro forma estimate of book value as of today, given the subsequent material increase in value of Toyota Industries’ stakes in publicly traded companies and in the overall Japanese stock market.
- Less than 1x EBITDA for the core operating business: At the Revised TOB price, Toyota Fudosan would effectively be acquiring the core operating business at a valuation of less than 1x EBITDA (see Appendix 5), resulting in ¥2.2 trillion of value accruing to Toyota Fudosan that instead should accrue to Toyota Industries’ shareholders.
The market appears to share our assessment. Toyota Industries’ shares have traded above the Revised TOB price since the January 14, 2026 announcement, indicating continued investor dissatisfaction with the transaction terms.
A Coercive Transaction
The fundamental conflicts and inherent coercion that arise from the Revised TOB and network of interconnected Toyota Group transactions call for enhanced transparency and adherence to the fundamental protections and fairness measures for minority shareholders. These are enshrined in the Fair M&A Guidelines, the Guidelines for Corporate Takeovers, and the Code of Corporate Conduct in the Securities Listing Regulation. Instead, the Revised TOB disregards many of the core principles underpinning these frameworks, including:
- Lack of true majority-of-minority protection: The Company claims the Revised TOB satisfies a majority-of-minority standard because the Toyota Group companies – which are clearly interested parties in the transaction – have not entered into binding agreements to tender their shares. This claim is disingenuous. On the one hand, the Company claims that these Toyota affiliates are independent. On the other, it rejected a legally binding offer from a third party to purchase the Company’s cross-shareholding in one of these Toyota affiliates at a higher price on the basis that selling the stake would jeopardize the Revised TOB.7 Under the currently proposed majority-of-minority condition, only 42% of non-Toyota Group shareholders need to tender into the Revised TOB, which is meaningfully below a true majority-of-minority threshold (see Appendix 6).
- Financial advisors that lack independence: Mitsubishi UFJ Morgan Stanley Securities and SMBC Nikko Securities – financial advisors to the Special Committee and the Company, respectively – are affiliated with entities that are key lenders to the offeror group, creating a clear conflict of interest.
- Abuse of minority shareholders to benefit Toyota Group companies: Toyota Industries has over-invested in its automobile business for years, as evidenced by exceptionally high capital intensity compared to peers and a bloated nearly ¥1 trillion asset base in this division, combined with an unacceptable low-single-digit return on invested capital. While this business is critical to the operations of Toyota Motor Corporation, it does not serve the best interests of Toyota Industries’ shareholders.
The Standalone Plan for Toyota Industries
We have been discussing a standalone plan for the Company (the “Standalone Plan”) with members of the Company’s Board and Special Committee for several months. The Standalone Plan represents a clear alternative to the Revised TOB that will generate significantly more value for Toyota Industries’ shareholders. The Company holds the number-one global position in forklifts, with 28% market share, and has a world-class automation systems business with attractive growth prospects. Toyota Industries also has substantial financial assets, a strong balance sheet and significant opportunities for operational improvement.
Elliott sees a clear path for Toyota Industries to achieve a valuation of more than ¥40,000 per share by 2028 through the Standalone Plan. Key elements of the Standalone Plan include:
- Unwinding cross-shareholdings outside the context of any tender offer;
- Capturing the significant margin improvement opportunity in the business, through consolidation initiatives, product revitalisation and increased efficiency;
- Improving capital allocation by ceasing overinvestment in the automotive segment, which today predominantly serves the interests of Toyota Motor Corporation rather than Toyota Industries, as well as other initiatives; and
- Implementing governance reforms to ensure Toyota Industries operates for the benefit of its own shareholders rather than other Toyota Group stakeholders.
The choice for Toyota Industries’ shareholders is not between accepting ¥18,800 or receiving less. It is between accepting ¥18,800 today or retaining ownership in a strong business capable of delivering more than twice that value over the medium term. Elliott plans to release further details of the Standalone Plan in the near future.
Do Not Tender
Elliott has no intention of tendering its shares into the Revised TOB and we strongly encourage other shareholders not to tender.
Based on our analysis, the Revised TOB significantly undervalues the Company and is not in the best interests of shareholders. Toyota Industries’ recent trading price suggests the broader market agrees. With a clear path to unlocking value as a standalone company through operational improvements and more efficient capital allocation, there is no imperative to proceed with this transaction. As a supportive long-term shareholder, we believe the Company has immense value-creation potential.
Even absent the implementation of the Standalone Plan, we believe that the Toyota Industries share price would, in the near term, significantly increase above its current levels if the Revised TOB fails, because the share price has been materially anchored down by the Original and Revised TOBs ever since the June 3, 2025 pre-announcement.
The outcome of this tender offer depends on the decisions of genuinely independent shareholders. If a sufficient number decide not to tender, the offer will not succeed at this price. Independent shareholders have the opportunity to determine whether they receive fair value for their investment – either through meaningfully improved transaction terms or through the Company pursuing a standalone path.
The implications of this transaction are far-reaching. If the Revised TOB is allowed to succeed, it will result in a substantial and potentially irreversible setback for Japan’s corporate governance reforms and dampen investor interest in the Japanese market. As one of the largest and most important corporate groups in Japan, how the Toyota Group acts will set the tone for how both domestic and foreign investors view the Japanese market. Every shareholder has a voice in this transaction and can affect its outcome. We urge you to advocate for a better outcome for Toyota Industries and its shareholders by declining to tender your shares.
Sincerely,
Aaron Tai
Portfolio ManagerGordon Singer
Managing PartnerDISCLAIMER
This document has been issued by Elliott Advisors (UK) Limited (“EAUK”), which is authorized and regulated by the United Kingdom’s Financial Conduct Authority (“FCA”), and Elliott Investment Management L.P. (“EIMLP”). Nothing within this document promotes, or is intended to promote, and may not be construed as promoting, any funds advised directly or indirectly by EAUK and EIMLP (the “Elliott Funds”).
This document is for discussion and informational purposes only. The views expressed herein represent the opinions of EAUK, EIMLP and their affiliates (collectively, “Elliott Management”) as of the date hereof. Elliott Management reserves the right to change or modify any of its opinions expressed herein at any time and for any reason and expressly disclaims any obligation to correct, update or revise the information contained herein or to otherwise provide any additional materials.
All of the information contained herein is based on publicly available information with respect to Toyota Industries Corporation (the “Company”), including public filings and disclosures made by the Company and other sources, as well as Elliott Management’s analysis of such publicly available information. Elliott Management has relied upon and assumed, without independent verification, the accuracy and completeness of all data and information available from public sources, and no representation or warranty is made that any such data or information is accurate. Elliott Management recognizes that there may be confidential or otherwise non-public information with respect to the Company that could alter the opinions of Elliott Management were such information known.
No representation, warranty or undertaking, express or implied, is given and no responsibility or liability or duty of care is or will be accepted by Elliott Management or any of its directors, officers, employees, agents, or advisors (each an “Elliott Person”) concerning: (i) this document and its contents, including whether the information and opinions contained herein are accurate, fair, complete or current; (ii) the provision of any further information, whether by way of update to the information and opinions contained in this document or otherwise to the recipient after the date of this document; or (iii) that Elliott Management’s investment processes or investment objectives will or are likely to be achieved or successful or that Elliott Management’s investments will make any profit or will not sustain losses. Past performance is not indicative of future results. To the fullest extent permitted by law, none of the Elliott Persons will be responsible for any losses, whether direct, indirect or consequential, including loss of profits, damages, costs, claims or expenses relating to or arising from the recipient’s or any person’s reliance on this document.
Except for the historical information contained herein, the information and opinions included in this document constitute forward-looking statements, including estimates and projections prepared with respect to, among other things, the Company’s anticipated operating performance, the value of the Company’s securities, debt or any related financial instruments that are based upon or relate to the value of securities of the Company (collectively, “Company Securities”), general economic and market conditions and other future events. You should be aware that all forward-looking statements, estimates and projections are inherently uncertain and subject to significant economic, competitive, and other uncertainties and contingencies and have been included solely for illustrative purposes. Actual results may differ materially from the information contained herein due to reasons that may or may not be foreseeable. There can be no assurance that the Company Securities will trade at the prices that may be implied herein, and there can be no assurance that any estimate, projection or assumption herein is, or will be proven, correct.
This document is for informational purposes only, and does not constitute (a) an offer or invitation to buy or sell, or a solicitation of an offer to buy or sell or to otherwise engage in any investment business or provide or receive any investment services in respect of, any security or other financial instrument and no legal relations shall be created by its issue, (b) a “financial promotion” for the purposes of the Financial Services and Markets Act 2000 of the U.K. (as amended), (c) “investment advice” as defined by the FCA’s Handbook of Rules and Guidance (“FCA Handbook”), (d) “investment research” as defined by the FCA Handbook, (e) an “investment recommendation” as defined by Regulation (EU) 596/2014 and by Regulation (EU) No. 596/2014 as it forms part of U.K. domestic law by virtue of section 3 of the European Union (Withdrawal) Act 2018 (“EUWA 2018”) including as amended by regulations issued under section 8 of EUWA 2018, (f) any action constituting “investment advisory business” as defined in Article 28, Paragraph 3, Item 1 of the Financial Instruments and Exchange Law of Japan (the “FIEL”), (g) any action constituting “investment management business” as defined in Article 28, Paragraph 4 of the FIEL, or (h) financial promotion, investment advice or an inducement or encouragement to participate in any product, offering or investment. No information contained herein should be construed as a recommendation by Elliott Management. This document is not intended to form the basis of any investment decision or as suggesting an investment strategy. This document is not (and may not be construed to be) legal, tax, investment, financial or other advice. Each recipient should consult their own legal counsel and tax and financial advisors as to legal and other matters concerning the information contained herein. This document does not purport to be all-inclusive or to contain all of the information that may be relevant to an evaluation of the Company, Company Securities or the matters described herein.
No agreement, commitment, understanding or other legal relationship exists or may be deemed to exist between or among Elliott Management and any other person by virtue of furnishing this document. Elliott Management is not acting for or on behalf of, and is not providing any advice or service to, any recipient of this document. Elliott Management is not responsible to any person for providing advice in relation to the subject matter of this document. Before determining on any course of action, any recipient should consider any associated risks and consequences and consult with its own independent advisors as it deems necessary.
The Elliott Funds may have a direct or indirect investment in the Company. Elliott Management therefore has a financial interest in the profitability of the Elliott Funds’ positions in the Company. Accordingly, Elliott Management may have conflicts of interest and this document should not be regarded as impartial. Nothing in this document should be taken as any indication of Elliott Management’s current or future trading or voting intentions which may change at any time. Elliott Management reserves the right to change its voting intention at any time notwithstanding any statements in this document.
Elliott Management intends to review its investments in the Company on a continuing basis and depending upon various factors, including without limitation, the Company’s financial position and strategic direction, the outcome of any discussions with the Company, overall market conditions, other investment opportunities available to Elliott Management, and the availability of Company Securities at prices that would make the purchase or sale of Company Securities desirable, Elliott Management may from time to time (in the open market or in private transactions, including since the inception of Elliott Management’s position) buy, sell, cover, hedge or otherwise change the form or substance of any of its investments (including Company Securities) to any degree in any manner permitted by law and expressly disclaims any obligation to notify others of any such changes. Elliott Management also reserves the right to take any actions with respect to its investments in the Company as it may deem appropriate.
Elliott Management has not sought or obtained consent from any third party to use any statements or information contained herein. Any such statements or information should not be viewed as indicating the support of such third party for the views expressed herein. All trademarks and trade names used herein are the exclusive property of their respective owners.
About Elliott
Elliott Investment Management L.P. (together with its affiliates, “Elliott”) manages approximately $76.1 billion of assets as of June 30, 2025. Founded in 1977, it is one of the oldest funds under continuous management. The Elliott funds’ investors include pension plans, sovereign wealth funds, endowments, foundations, funds-of-funds, high net worth individuals and families, and employees of the firm. Elliott Advisors (UK) Limited is an affiliate of Elliott Investment Management L.P.
Investor Contacts:
Okapi Partners LLC
New York: Pat McHugh
T:+1 212 297 0720
Toll Free: (877) 629-6357
London: Christian Jacques
T: +44 20 3031 6613
[email protected]Media Contacts:
London
Stijn van de Grampel
Elliott Advisors (UK) Limited
T: +44 20 3009 1061
[email protected]New York
Stephen Spruiell
Elliott Investment Management L.P.
T: +1 (212) 478-2017
[email protected]Tokyo
Brett Wallbutton
Ashton Consulting
T: +81 (0) 3 5425-7220
[email protected]
1 Based on Toyota Industries’ semi-annual report for the period ended September 30, 2025 and other public sources of information, we believe Elliott is the largest shareholder of Toyota Industries which is not affiliated with any Toyota Group companies.
2 The “Fair M&A Guidelines ― Enhancing Corporate Value and Securing Shareholders’ Interests” published by the Ministry of Economy, Trade and Industry dated June 28, 2019.
3 The “Guidelines for Corporate Takeovers – Enhancing Corporate Value and Securing Shareholders’Interests” published by the Ministry of Economy, Trade and Industry dated August 31, 2023.
4 The “Revisions to Securities Listing Regulations and Other Rules Pertaining to MBOs and Subsidiary Conversions” published by the Tokyo Stock Exchange dated July 7, 2025.
5 At a tax rate reflecting the benefits to Toyota Industries from its larger cross-shareholdings from the deemed dividend tax treatment under the issuer buyback unwind structure the Company plans to utilize.
6 Appendix 7 (The Process of Negotiations Before the Report) to the Toyota Industries Special Committee report dated January 14, 2026.
7 Page 35 of the Toyota Industries Special Committee report dated January 14, 2026.
SOURCE Elliott Investment Management L.P.
Continue Reading
-

Trump Tariff Threats Weigh on Asian Risk Appetite: Markets Wrap
(Bloomberg) — Asian markets are facing some pressure early Monday after US President Donald Trump proposed new tariffs on eight European countries, denting risk appetite and boosting demand for haven assets.
The pound and euro led losses among Group-of-10 currencies against the dollar in early trading, while the yen and Swiss franc edged higher. Equity futures point to declines in Japan and Hong Kong and little change in Australia when markets reopen, after US shares inched lower on Friday.
Trump said over the weekend he’d impose a 10% tariff on goods from eight European countries starting Feb. 1, rising to 25% in June unless there’s a deal for a “purchase of Greenland.” The move drew quick rebukes from European leaders, who are now poised to halt the approval of the trade agreement struck last year. Bloomberg reported that French President Emmanuel Macron may request the activation of the EU’s anti-coercion instrument – the bloc’s most powerful retaliation tool.
“The outcome of these new trade tensions is unclear, but what has long been evident is that there is no such thing as trade or tariff certainty anymore,” analysts including Carsten Brzeski, global head of macro at ING Bank, wrote in a note to clients. “What is clear is that a full-blown trade war between the EU and the US would leave only losers.”
Asian assets were already facing pressure after US stocks on Friday gave up an earlier gain to close 0.1% lower, after Trump suggested he’d nominated someone other than Kevin Hassett to succeed Fed Chair Jerome Powell. Treasuries slid across the curve as traders dialed back expectations for rate cuts, with odds lifted that former Fed Governor Kevin Warsh will be nominated to lead the Fed.
Chinese data on Monday may show the economy remained sanguine in the fourth quarter and likely capped 2025 with its weakest quarterly growth in three years. Gross domestic product is expected to gain 4.5% year-on-year in the three months to Dec. 31, slower than the 4.8% in the prior quarter, according to a Bloomberg survey.
Eyes will then shift to the European open, with the region’s equities likely to bare the brunt of any selloff, according to strategists. Deutsche Bank anticipates the fallout on the euro may ultimately be limited given the US relies on Europe for capital, while others see Trump’s salvo purely as a negotiating tactic to gain leverage ahead of the World Economic Forum at Davos this week.
“My working assumption is that an ‘off ramp’ from these threats will soon be found, and that this turns into yet another ‘TACO moment’,” Michael Brown, a strategist at Pepperstone Group in London, wrote in a note to clients. “With the fundamental bull case for risk still a resilient one, and providing that any European retaliation remains largely rhetorical, I would view equity dips as buying opportunities for now and wouldn’t be surprised to see the week’s initial FX moves fade relatively rapidly.”
In commodities, oil edged higher Friday to settle near $60 a barrel as traders weighed tensions in Iran. Gold slipped the most in two weeks.
Some of the main moves in markets:
Currencies
The Japanese yen rose 0.2% to 157.89 per dollar as of 7:00 a.m. Tokyo time The euro fell 0.1% to $1.1584 The Australian dollar fell 0.1% to $0.6674 The offshore yuan was little changed at 6.9662 per dollar Bonds
Australia’s 10-year yield advanced three basis points to 4.73% Cryptocurrencies
Bitcoin was little changed at $95,343.95 Ether rose 0.8% to $3,337.5 ©2026 Bloomberg L.P.
Continue Reading
-
Monolithic Power Systems (MPWR) Emerges as High-Conviction AI Data Center Power Play
We recently compiled a list of the 10 Best Investments During A Recession. Monolithic Power Systems, Inc. is placed ninth among the best investments.
TheFly reported on December 19, 2025, that Truist Securities raised its price target for MPWR to $1,375 from $1,163 while maintaining a Buy rating. The company’s strength, according to analyst William Stein, is a compelling AI infrastructure derivative bet, which is fueled by its expertise in high-density power delivery for next-generation GPU and XPU platforms that support a multibillion-dollar potential in AI data centers.
Monolithic Power Systems, Inc. (MPWR) Emerges as High-Conviction AI Data Center Power Play Monolithic Power Systems, Inc. (NASDAQ:MPWR) designs, develops, and markets integrated circuits (ICs) for the computing, automotive, industrial, and communications markets. The company specializes in power management solutions that reduce total energy consumption and heat dissipation in high-performance environments.
While we acknowledge the potential of MPWR as an investment, we believe certain AI stocks offer greater upside potential and carry less downside risk. If you’re looking for an extremely undervalued AI stock that also stands to benefit significantly from Trump-era tariffs and the onshoring trend, see our free report on the best short-term AI stock.
READ NEXT: 12 Best Multibagger Stocks to Buy Heading into 2026 and 7 Best Rising Tech Stocks to Buy Now.
Disclosure: None.
Continue Reading
-

We Ran A Stock Scan For Earnings Growth And Scales (NZSE:SCL) Passed With Ease
Investors are often guided by the idea of discovering ‘the next big thing’, even if that means buying ‘story stocks’ without any revenue, let alone profit. Unfortunately, these high risk investments often have little probability of ever paying off, and many investors pay a price to learn their lesson. Loss-making companies are always racing against time to reach financial sustainability, so investors in these companies may be taking on more risk than they should.
So if this idea of high risk and high reward doesn’t suit, you might be more interested in profitable, growing companies, like Scales (NZSE:SCL). While profit isn’t the sole metric that should be considered when investing, it’s worth recognising businesses that can consistently produce it.
Trump has pledged to “unleash” American oil and gas and these 15 US stocks have developments that are poised to benefit.
The market is a voting machine in the short term, but a weighing machine in the long term, so you’d expect share price to follow earnings per share (EPS) outcomes eventually. So it makes sense that experienced investors pay close attention to company EPS when undertaking investment research. It certainly is nice to see that Scales has managed to grow EPS by 26% per year over three years. If growth like this continues on into the future, then shareholders will have plenty to smile about.
It’s often helpful to take a look at earnings before interest and tax (EBIT) margins, as well as revenue growth, to get another take on the quality of the company’s growth. Scales shareholders can take confidence from the fact that EBIT margins are up from 10% to 13%, and revenue is growing. Both of which are great metrics to check off for potential growth.
You can take a look at the company’s revenue and earnings growth trend, in the chart below. For finer detail, click on the image.
NZSE:SCL Earnings and Revenue History January 18th 2026 See our latest analysis for Scales
The trick, as an investor, is to find companies that are going to perform well in the future, not just in the past. While crystal balls don’t exist, you can check our visualization of consensus analyst forecasts for Scales’ future EPS 100% free.
It’s said that there’s no smoke without fire. For investors, insider buying is often the smoke that indicates which stocks could set the market alight. That’s because insider buying often indicates that those closest to the company have confidence that the share price will perform well. However, insiders are sometimes wrong, and we don’t know the exact thinking behind their acquisitions.
Continue Reading
-

High Roller Technologies (ROLR) Is Up 541.8% After Crypto.com Prediction Markets Pact
-
In mid-January 2026, High Roller Technologies, Inc. announced a binding Letter of Intent with Crypto.com | Derivatives North America to power an exclusive, regulated U.S. event-based prediction markets platform spanning finance, entertainment, and sports via HighRoller.com.
-
Layered on top of this core infrastructure deal, High Roller is lining up large social and sports media partners to funnel already-engaged, prediction-focused audiences into its upcoming U.S. prediction markets offering.
-
Against this backdrop, we’ll explore how the Crypto.com-powered, regulated prediction markets launch could reshape High Roller’s investment narrative.
AI is about to change healthcare. These 109 stocks are working on everything from early diagnostics to drug discovery. The best part – they are all under $10b in market cap – there’s still time to get in early.
To own High Roller today, you have to believe it can evolve from a small, volatile iGaming operator into a regulated prediction-markets gateway, using Crypto.com’s CFTC-registered infrastructure and a web of social-first media partners to pull in already-engaged, odds-literate users. The binding LOI with Crypto.com, alongside LOIs with Forever Network, Leverage Game Media, and Spike Up Media’s Lines.com, shifts the near-term catalyst set toward execution: securing definitive agreements, hitting the targeted HighRoller.com launch, and proving that these large audience funnels can translate into compliant, paying customers. At the same time, the stock’s very large recent re-rating, thin balance sheet, and unprofitable history keep valuation risk and funding needs front and center. The recent news adds credible distribution and product story, but also raises the bar for delivery.
But against that excitement, one near term risk stands out that investors should not ignore. Our valuation report here indicates High Roller Technologies may be overvalued.
ROLR 1-Year Stock Price Chart Explore another fair value estimate on High Roller Technologies – why the stock might be worth as much as $15.57!
Disagree with this assessment? Create your own narrative in under 3 minutes – extraordinary investment returns rarely come from following the herd.
-
A great starting point for your High Roller Technologies research is our analysis highlighting 2 important warning signs that could impact your investment decision.
-
Our free High Roller Technologies research report provides a comprehensive fundamental analysis summarized in a single visual – the Snowflake – making it easy to evaluate High Roller Technologies’ overall financial health at a glance.
Continue Reading
-
-

Europe can wield a $8 trillion ‘sell America’ weapon as Trump reignites a trade war over Greenland
As the European Union weighs options to retaliate against President Donald Trump’s latest tariffs, its most potent weapon may be in financial markets.
France is already urging the EU to deploy its “anti-coercion instrument,” which can target foreign direct investment and finance as well as trade. That’s after Trump announced new U.S. tariffs on NATO countries that sent troops to Greenland amid his plans to take over the semi-autonomous Danish territory.
At face value, a 10% tariff rising to 25% would have minimal economic consequences, Capital Economics chief economist Neil Shearing said in a note Sunday, estimating they would reduce GDP in the targeted NATO economies by 0.1-0.3 percentage points and add 0.1-0.2 points to U.S. inflation.
“The political ramifications would be far greater than the economic ones,” he warned, with any attempt by the U.S. to seize Greenland by force or coercion potentially leading to irreparable harm to NATO.
So far, European officials have signaled Greenland’s sovereignty is a red line that’s not up for compromise, while the Trump administration isn’t budging either on its stance.
But the U.S. has a key vulnerability the EU can exploit, according to George Saravelos, head of FX research at Deutsche Bank.
“Europe owns Greenland, it also owns a lot of Treasuries,” he wrote in a note on Sunday.
Holding those bonds helps balance America’s massive external deficits, and Europe is the world’s biggest lender to the U.S.
For example, offsetting the U.S. trade imbalance requires heavy inflows of capital from abroad. Meanwhile, the Treasury Department must also finance budget gaps by issuing more debt, often to foreign investors.
“European countries own $8 trillion of US bonds and equities, almost twice as much as the rest of the world combined,” Saravelos pointed out. “In an environment where the geoeconomic stability of the western alliance is being disrupted existentially, it is not clear why Europeans would be as willing to play this part.”
As Trump threatened to upend global trade and finance last year, Danish pension funds led the charge in reducing their dollar exposure and repatriating money back home, he said.
Such moves represented the “sell America” trade that saw investors dump dollar-denominated assets amid doubts that they would continue serving as safe havens or still deliver attractive returns.
“With USD exposure still very elevated across Europe, developments over the last few days have potential to further encourage dollar rebalancing,” Saravelos added.
At the same time, the euro and Danish krone may see minimal impact from the fallout of Trump’s tariffs on NATO and any subsequent retaliation, he predicted.
That’s as European political cohesion stands to solidify in the face of Trump’s threats, with even right-wing officials previously sympathetic to him now rejecting his heavy-handed approach.
Saravelos sees additional leverage for Europe ahead of U.S. midterm elections with the Trump administration focused on affordability issues. On that front, the EU could influence inflation and Treasury yields, which affect borrowing costs.
“With the US net international investment position at record negative extremes, the mutual inter-dependence of European-US financial markets has never been higher,” he said. “It is a weaponization of capital rather than trade flows that would by far be the most disruptive to markets.”
Continue Reading
-

Horse massage firm warned after using Welsh government logo on fake diplomas
A company selling fake diplomas for people to give massages to horses was one of six firms caught by the Welsh government for using their dragon logo without permission.
Those who received the fraudulent certificates from the “equine massage service” were instructed to destroy them, and government officials sent cease and desist letters to the firm’s owners.
The government in Cardiff found 10 cases of their logo being used without permission since 2020, which the BBC obtained using a Freedom of Information request.
A government spokesperson said it took the integrity of its brand “very seriously” and took “robust action against any improper use”.
The Welsh government refused to tell the BBC the names of the six companies that were sent cease and desist letters to stop the misuse, nor would they say whether police were contacted.
But the one teaching people to give therapy to horses was found to be issuing fraudulent diplomas which displayed the logo in 2022.
A cease and desist letter was issued by the Welsh government, the genuine awarding body for equine massage therapy took up the matter with the service, and all learners were instructed to destroy their certificates.
Elsewhere, three companies were found to be selling fake diplomas displaying the logo in 2020, and three fake accounts were set up on Instagram carrying the logo in 2022 – which Instagram removed once contacted.
The same year, an applicant for a job with a catering firm had submitted a fake certificate demonstrating pool supervision skills which displayed the logo – but he was ordered to destroy it by the awarding body after the government was alerted.
In 2023, a company offering energy efficiency services used the logo without permission in Facebook adverts, and in 2024 another company selling fake diplomas was sent a cease and desist letter and the website was taken down.
A government spokesperson said: “It is important that citizens can trust information provided by the government under its branding.
“We continuously monitor this and where necessary take robust action against any improper use by third parties.”
The Welsh government expects its logo, created in May 2011, to be used on publications and materials where it is a significant contributor to schemes.
Its guidance says: “Our achievements matter to us, and we are proud to add our logo to all projects we are involved in, for example whether it’s improving a community centre, building a new school, a hospital wing, improving roads or the surroundings of train stations.”
It also says “our logo is a dragon and bilingual title, separated by a horizontal line.
“These elements are in a fixed relationship to each other, which must not be altered in any way.
“Our logo colour is either black or white. No other colour is permitted.”
There were eight cases of the logo being used without permission over the previous five years, including a company offering embroidered images of the ministerial dragon for sale.
Continue Reading