THE WOODLANDS, Texas, Dec. 1, 2025 /PRNewswire/ — Huntsman Corporation (NYSE: HUN) is currently experiencing an unplanned outage at its Polyurethanes facility located in Rotterdam, Netherlands which will likely have a negative impact on fourth quarter 2025 adjusted EBITDA of approximately $10 million. The larger of the two MDI lines at the facility is impacted and is expected to resume production by mid-December. As a result of the outage, Management currently expects the fourth quarter 2025 adjusted EBITDA to be at the low end of the $25 million to $50 million range communicated on November 6, 2025. Excluding the outage the quarter is trending as previously expected.
About Huntsman: Huntsman Corporation is a publicly traded global manufacturer and marketer of differentiated and specialty chemicals with 2024 revenues of approximately $6 billion. Our chemical products number in the thousands and are sold worldwide to manufacturers serving a broad and diverse range of consumer and industrial end markets. We operate more than 60 manufacturing, R&D and operations facilities in approximately 25 countries and employ approximately 6,300 associates within our continuing operations. For more information about Huntsman, please visit the company’s website at www.huntsman.com.
Social Media: X: www.x.com/Huntsman_Corp Facebook: www.facebook.com/huntsmancorp LinkedIn: www.linkedin.com/company/huntsman
Forward-Looking Statements: Certain information in this release constitutes forward-looking statements within the meaning of Section 27A of the Securities Act of 1933 and Section 21E of the Securities Exchange Act of 1934. These statements are based on management’s current beliefs and expectations. The forward-looking statements in this release are subject to uncertainty and changes in circumstances and involve risks and uncertainties that may affect the company’s operations, markets, products, services, prices and other factors as discussed under the caption “Risk Factors” in the Huntsman companies’ filings with the U.S. Securities and Exchange Commission. Significant risks and uncertainties may relate to, but are not limited to, volatile global economic conditions, cyclical and volatile product markets, disruptions in production at manufacturing facilities, reorganization or restructuring of Huntsman’s operations, including any delay of, or other negative developments affecting the ability to implement cost reductions, timing of proposed transactions, and manufacturing optimization improvements in Huntsman businesses and realize anticipated cost savings, and other financial, economic, competitive, environmental, political, legal, regulatory and technological factors. The company assumes no obligation to provide revisions to any forward-looking statements should circumstances change, except as otherwise required by applicable laws.
View original content to download multimedia:https://www.prnewswire.com/news-releases/huntsman-updates-fourth-quarter-2025-outlook-302629501.html
Atlas Revenue up 30% year-over-year; 75% of Total Q3 Revenue
Third Quarter Fiscal 2026 Total Revenue of $628.3 million, up 19% year-over-year
Added 2,600 Customers, with Over 62,500 Total Customers as of October 31, 2025
NEW YORK, Dec. 1, 2025 /PRNewswire/ — MongoDB, Inc. (NASDAQ: MDB) today announced its financial results for the third quarter ended October 31, 2025.
“MongoDB delivered strong third quarter results that exceeded the high-end of our guidance driven by continued strength in Atlas, which saw growth accelerate to 30% year-over-year. We also delivered meaningful margin outperformance as we executed on our plan to drive profitable growth. Reflecting this strength, we are raising our guidance on the top and bottom line for the rest of the year,” said CJ Desai, President and Chief Executive Officer of MongoDB.
“Q3 was an exceptional quarter. Existing customers are expanding with us and net-new customer additions continue to show strength. Companies across industries and geographies are choosing MongoDB because we provide a unified data platform that powers mission-critical workloads today and also positions them to capitalize on the emerging AI platform shift.”
Third Quarter Fiscal 2026 Financial Highlights
Revenue: Total revenue was $628.3 million for the third quarter of fiscal 2026, an increase of 19% year-over-year. Subscription revenue was $609.1 million, an increase of 19% year-over-year, and services revenue was $19.2 million, an increase of 12% year-over-year.
Gross Profit: Gross profit was $449.1 million for the third quarter of fiscal 2026, representing a 71% gross margin compared to 74% in the year-ago period. Non-GAAP gross profit was $466.2 million, representing a 74% non-GAAP gross margin, compared to a non-GAAP gross margin of 77% in the year-ago period.
Loss from Operations: Loss from operations was $18.4 million for the third quarter of fiscal 2026, compared to a loss from operations of $27.9 million in the year-ago period. Non-GAAP income from operations was $123.1 million, compared to non-GAAP income from operations of $101.5 million in the year-ago period.
Net Loss: Net loss was $2.0 million, or $0.02 per share, based on 81.4 million weighted-average shares outstanding, for the third quarter of fiscal 2026. This compares to a net loss of $9.8 million, or $0.13 per share, in the year-ago period. Non-GAAP net income was $114.5 million, or $1.32 per share, based on 86.9 million fully diluted weighted-average shares outstanding. This compares to a non-GAAP net loss of $98.1 million, or $1.16, per share in the year-ago period.
Cash Flow: As of October 31, 2025, MongoDB had $2.3 billion in cash, cash equivalents, short-term investments and restricted cash. During the three months ended October 31, 2025, MongoDB generated $143.5 million of cash from operations, compared to $37.4 million of cash from operations in the year-ago period. MongoDB used $1.7 million of cash in capital expenditures and used $1.7 million of cash in principal payments of finance leases, leading to free cash flow of $140.1 million, compared to free cash flow of $34.6 million in the year-ago period.
A reconciliation of each non-GAAP measure to the most directly comparable GAAP measure has been provided in the financial statement tables included at the end of this press release. An explanation of these measures is also included below under the heading “Non-GAAP Financial Measures.”
Third Quarter Fiscal 2026 and Recent Business Highlights
MongoDB appointed Chirantan “CJ” Desai as President and Chief Executive Officer, succeeding Dev Ittycheria, who held the role for 11 years. CJ comes to MongoDB with an exceptional blend of product and engineering leadership, strong go-to-market execution, and firsthand experience scaling some of the world’s most transformative software companies.
MongoDB has been recognized as a Leader for the fourth consecutive year in the 2025 Gartner® Magic Quadrant™ for Cloud Database Management Systems (CDBMS). This recognition reflects the company’s execution strength, innovation velocity, and continued leadership in redefining what a modern database platform can do in the era of AI. Our placement underscores MongoDB’s position as the trusted foundation for enterprises seeking agility, scalability, and AI readiness across every application.
MongoDB announced the availability of its search and vector search capabilities within MongoDB Community Edition and MongoDB Enterprise Server. Previously exclusive to the fully managed MongoDB Atlas cloud platform, developers and organizations of all sizes can now access the preview of robust full-text search and vector search capabilities on MongoDB’s local, on-premises, and self-managed offerings—all with the world’s most popular modern database.
MongoDB was named the 2025 Microsoft United States Partner of the Year at the Microsoft Ignite conference in San Francisco. MongoDB also launched a number of AI development, security, and governance technology integrations with Microsoft that solidify MongoDB’s position as the best data foundation for AI on Microsoft Azure.
Fourth Quarter and Full Year Fiscal 2026 Guidance
Based on information available to management as of today, December 1, 2025, MongoDB is issuing the following financial guidance for the fourth quarter and full year fiscal 2026.
Fourth Quarter Fiscal 2026
Full Year Fiscal 2026
Revenue
$665.0 million to $670.0
million
$2.434 billion to $2.439 billion
Non-GAAP Income from Operations
$139.0 million to $143.0 million
$436.4 million to $440.4 million
Non-GAAP Net Income per Share
$1.44 to $1.48
$4.76 to $4.80
Reconciliations of non-GAAP income from operations and non-GAAP net income per share guidance to the most directly comparable GAAP measures are not available without unreasonable efforts on a forward-looking basis due to the high variability, complexity and low visibility with respect to the charges excluded from these non-GAAP measures; in particular, the measures and effects of stock-based compensation expense specific to equity compensation awards that are directly impacted by unpredictable fluctuations in MongoDB’s stock price. MongoDB expects the variability of the above charges to have a significant, and potentially unpredictable, impact on its future GAAP financial results.
Conference Call Information
MongoDB will host a conference call today, December 1, 2025, at 5:00 p.m. (Eastern Time) to discuss its financial results and business outlook. A live webcast of the call will be available on the “Investor Relations” page of MongoDB’s website at https://investors.mongodb.com. To access the call by phone, please go to this link (registration link), and you will be provided with dial in details. To avoid delays, we encourage participants to dial into the conference call fifteen minutes ahead of the scheduled start time. A replay of the webcast will also be available for a limited time at http://investors.mongodb.com.
Forward-Looking Statements
This press release includes certain “forward-looking statements” within the meaning of Section 27A of the Securities Act of 1933, as amended, or the Securities Act, and Section 21E of the Securities Exchange Act of 1934, as amended, including statements concerning MongoDB’s financial guidance for the fourth fiscal quarter and full year fiscal 2026. These forward-looking statements include, but are not limited to, plans, objectives, expectations and intentions and other statements contained in this press release that are not historical facts and statements identified by words such as “anticipate,” “believe,” “continue,” “could,” “estimate,” “expect,” “intend,” “may,” “plan,” “project,” “will,” “would” or the negative or plural of these words or similar expressions or variations. These forward-looking statements reflect our current views about our plans, intentions, expectations, strategies and prospects, which are based on the information currently available to us and on assumptions we have made. Although we believe that our plans, intentions, expectations, strategies and prospects as reflected in or suggested by those forward-looking statements are reasonable, we can give no assurance that the plans, intentions, expectations or strategies will be attained or achieved. Furthermore, actual results may differ materially from those described in the forward-looking statements and are subject to a variety of assumptions, uncertainties, risks and factors that are beyond our control including, without limitation: our customers renewing their subscriptions with us and expanding their usage of software and related services; global political changes; the effects of the ongoing military conflicts between Russia and Ukraine and Israel and Hamas on our business and future operating results; economic downturns and/or the effects of rising interest rates, inflation and volatility in the global economy and financial markets on our business and future operating results; our potential failure to meet publicly announced guidance or other expectations about our business and future operating results; reputational harm or other adverse consequences resulting from use of AI and ML in our product offerings and internal operations if they don’t produce the desired benefits; our limited operating history; our history of losses; our potential failure to repurchase shares of our common stock at favorable prices, if at all; failure of our platform to satisfy customer demands; the effects of increased competition; our investments in new products and our ability to introduce new features, services or enhancements; social, ethical and security issues relating to the use of new and evolving technologies, such as artificial intelligence, in our offerings or partnerships; our ability to effectively expand our sales and marketing organization; our ability to continue to build and maintain credibility with the developer community; our ability to add new customers or increase sales to our existing customers; our ability to maintain, protect, enforce and enhance our intellectual property; the effects of social, ethical and regulatory issues relating to the use of new and evolving technologies, such as AI and ML, in our offerings or partnerships; the growth and expansion of the market for database products and our ability to penetrate that market; our ability to maintain the security of our software and adequately address privacy concerns; our ability to manage our growth effectively and successfully recruit and retain additional highly-qualified personnel; and the price volatility of our common stock. These and other risks and uncertainties are more fully described in our filings with the Securities and Exchange Commission (“SEC”), including under the caption “Risk Factors” in our Quarterly Report on Form 10-Q for the quarter ended July 31, 2025, filed with the SEC on August 27, 2025. Additional information will be made available in our Quarterly Report on Form 10-Q for the quarter ended October 31, 2025, and other filings and reports that we may file from time to time with the SEC. Except as required by law, we undertake no duty or obligation to update any forward-looking statements contained in this release as a result of new information, future events, changes in expectations or otherwise.
Non-GAAP Financial Measures
This press release includes the following financial measures defined as non-GAAP financial measures by the SEC: non-GAAP gross profit, non-GAAP gross margin, non-GAAP operating expenses, non-GAAP income from operations, non-GAAP operating margin, non-GAAP net income, non-GAAP net income per share and free cash flow. Non-GAAP gross profit and non-GAAP gross margin exclude expenses associated with stock-based compensation. Non-GAAP operating expenses, non-GAAP income from operations, non-GAAP operating margin, non-GAAP net income and non-GAAP net income per share exclude:
expenses associated with stock-based compensation including employer payroll taxes upon the vesting and exercising of stock-based awards and expenses related to stock appreciation rights previously issued to our employees in China;
amortization of intangible assets for the acquired technology and acquired customer relationships associated with prior acquisitions;
certain acquisition-related costs and other, including due diligence costs, professional fees in connection with an acquisition and certain integration-related expenses. These expenses are unpredictable, and dependent on factors that may be outside of our control and unrelated to the continuing operations of the acquired business or our Company. In addition, the size and complexity of an acquisition, which often drives the magnitude of acquisition-related costs, may not be indicative of such future costs;
restructuring costs associated with a formal restructuring plan that are primarily related to workforce reductions. The Company excludes these expenses because they are not reflective of ordinary course ongoing business and operating results; and
in the case of non-GAAP net income and non-GAAP net income per share, amortization of the debt issuance costs associated with our convertible senior notes and gains or losses on our financial instruments;
additionally, non-GAAP net income and non-GAAP net income per share are adjusted for an assumed provision for income taxes based on an estimated long-term non-GAAP tax rate. The non-GAAP tax rate was calculated utilizing a three-year financial projection that excludes the direct impact of the GAAP to non-GAAP adjustments and considers other factors such as operating structure and existing tax positions in various jurisdictions. We intend to periodically reevaluate the projected long-term tax rate, as necessary, for significant events and our ongoing analysis of relevant tax law changes.
MongoDB uses these non-GAAP financial measures internally in analyzing its financial results and believes they are useful to investors, as a supplement to GAAP measures, in evaluating MongoDB’s ongoing operational performance. MongoDB believes that the use of these non-GAAP financial measures provides an additional tool for investors to use in evaluating ongoing operating results and trends and in comparing its financial results with other companies in MongoDB’s industry, many of which may present similar non-GAAP financial measures to investors.
Free cash flow represents net cash from/used in operating activities, less capital expenditures, principal payments of finance lease liabilities and capitalized software development costs, if any. MongoDB uses free cash flow to understand and evaluate its liquidity and to generate future operating plans. The exclusion of capital expenditures, principal payments of finance lease liabilities and amounts capitalized for software development facilitates comparisons of MongoDB’s liquidity on a period-to-period basis and excludes items that it does not consider to be indicative of its liquidity. MongoDB believes that free cash flow is a measure of liquidity that provides useful information to investors in understanding and evaluating the strength of its liquidity and future ability to generate cash that can be used for strategic opportunities or investing in its business in the same manner as MongoDB’s management and board of directors.
Non-GAAP financial measures have limitations as an analytical tool and should not be considered in isolation from, or as a substitute for, financial information prepared in accordance with GAAP. In particular, other companies may report non-GAAP gross profit, non-GAAP gross margin, non-GAAP operating expenses, non-GAAP income from operations, non-GAAP net income, non-GAAP net income per share, free cash flow or similarly titled measures but calculate them differently, which reduces their usefulness as comparative measures. Investors are encouraged to review the reconciliation of these non-GAAP financial measures to their most directly comparable GAAP financial measures, as presented below. This earnings press release and any future releases containing such non-GAAP reconciliations can also be found on the Investor Relations page of MongoDB’s website at https://investors.mongodb.com.
About MongoDB
Headquartered in New York, MongoDB’s mission is to empower innovators to create, transform, and disrupt industries with software and data. MongoDB’s unified, intelligent data platform was built to power the next generation of applications, and MongoDB is the most widely available, globally distributed database on the market. With integrated capabilities for operational data, search, real-time analytics, and AI-powered retrieval, MongoDB helps organizations everywhere move faster, innovate more efficiently, and simplify complex architectures. Millions of developers and more than 60,000 customers across almost every industry—including 70% of the Fortune 100—rely on MongoDB for their most important applications. To learn more, visit mongodb.com.
Investor Relations
Jess Lubert
[email protected]
Media Relations
MongoDB
[email protected]
MONGODB, INC.
CONDENSED CONSOLIDATED BALANCE SHEETS
(in thousands of U.S. dollars, except share and per share data)
(unaudited)
October 31, 2025
January 31, 2025
Assets
Current assets:
Cash and cash equivalents
$ 834,092
$ 490,133
Short-term investments
1,471,669
1,846,444
Accounts receivable, net of allowance for doubtful accounts of $12,305 and $8,888 as of October 31, 2025 and January 31, 2025, respectively
416,494
393,099
Deferred commissions
122,882
112,632
Prepaid expenses and other current assets
87,177
81,214
Total current assets
2,932,314
2,923,522
Property and equipment, net
40,704
46,377
Operating lease right-of-use assets
30,914
34,607
Goodwill
189,641
69,679
Intangible assets, net
38,308
24,597
Deferred tax assets
23,012
20,810
Other assets
311,756
310,701
Total assets
$ 3,566,649
$ 3,430,293
Liabilities and Stockholders’ Equity
Current liabilities:
Accounts payable
$ 14,811
$ 10,467
Accrued compensation and benefits
131,760
120,354
Operating lease liabilities
9,145
9,126
Other accrued liabilities
101,444
87,659
Deferred revenue
300,873
334,381
Total current liabilities
558,033
561,987
Deferred tax liability
560
262
Operating lease liabilities
25,480
27,374
Deferred revenue
66,173
25,404
Other liabilities
27,964
33,042
Total liabilities
678,210
648,069
Stockholders’ equity:
Common stock, par value of $0.001 per share; 1,000,000,000 shares authorized as of October 31, 2025 and January 31, 2025; 82,919,928 shares issued and 81,357,418 shares outstanding as of October 31, 2025; 80,558,847 shares issued and 80,467,811 shares outstanding as of January 31, 2025
81
78
Additional paid-in capital
5,152,122
4,625,093
Treasury stock, 1,562,510 shares (repurchased at an average of $221.86 per share) as of October 31, 2025 and 99,371 shares (repurchased at an average of $13.27 per share) as of January 31, 2025
(346,654)
(1,319)
Accumulated other comprehensive income (loss)
10,275
(924)
Accumulated deficit
(1,927,385)
(1,840,704)
Total stockholders’ equity
2,888,439
2,782,224
Total liabilities and stockholders’ equity
$ 3,566,649
$ 3,430,293
MONGODB, INC.
CONDENSED CONSOLIDATED STATEMENTS OF OPERATIONS
(in thousands of U.S. dollars, except share and per share data)
(unaudited)
Three Months Ended October 31,
Nine Months Ended October 31,
2025
2024
2025
2024
Revenue:
Subscription
$ 609,067
$ 512,205
$ 1,712,877
$ 1,412,906
Services
19,242
17,170
55,848
45,139
Total revenue
628,309
529,375
1,768,725
1,458,045
Cost of revenue:
Subscription(1)
146,921
111,150
416,455
318,728
Services(1)
32,256
24,181
92,191
67,553
Total cost of revenue
179,177
135,331
508,646
386,281
Gross profit
449,132
394,044
1,260,079
1,071,764
Operating expenses:
Sales and marketing(1)
230,864
217,954
695,852
658,937
Research and development(1)
176,610
151,410
527,178
446,437
General and administrative(1)
60,082
52,556
174,321
163,892
Total operating expenses
467,556
421,920
1,397,351
1,269,266
Loss from operations
(18,424)
(27,876)
(137,272)
(197,502)
Other income, net
19,774
20,767
62,178
61,749
Income (loss) before provision for income taxes
1,350
(7,109)
(75,094)
(135,753)
Provision for income taxes
3,357
2,667
11,587
9,145
Net loss
$ (2,007)
$ (9,776)
$ (86,681)
$ (144,898)
Net loss per share, basic and diluted
$ (0.02)
$ (0.13)
$ (1.07)
$ (1.97)
Weighted-average shares used to compute net loss per share, basic and diluted
81,401,853
74,020,593
81,245,331
73,472,900
(1) Includes stock‑based compensation expense as follows:
Three Months Ended October 31,
Nine Months Ended October 31,
2025
2024
2025
2024
Cost of revenue—subscription
$ 8,990
$ 7,884
$ 26,216
$ 21,566
Cost of revenue—services
4,572
3,495
12,739
10,151
Sales and marketing
36,965
40,540
112,332
121,193
Research and development
67,255
57,850
208,773
168,211
General and administrative
15,848
15,943
46,401
47,777
Total stock‑based compensation expense
$ 133,630
$ 125,712
$ 406,461
$ 368,898
MONGODB, INC.
CONDENSED CONSOLIDATED STATEMENTS OF CASH FLOWS
(in thousands of U.S. dollars)
(unaudited)
Three Months Ended October 31,
Nine Months Ended October 31,
2025
2024
2025
2024
Cash flows from operating activities
Net loss
$ (2,007)
$ (9,776)
$ (86,681)
$ (144,898)
Adjustments to reconcile net loss to net cash provided by operating activities:
Depreciation and amortization
5,668
2,405
16,654
9,580
Stock-based compensation
133,630
125,712
406,461
368,898
Amortization of debt discount and issuance costs
—
715
—
2,419
Amortization of finance right-of-use assets
995
994
2,981
2,981
Amortization of operating right-of-use assets
2,899
3,229
8,498
8,300
Deferred income taxes
447
(825)
(687)
(799)
Amortization of premium and accretion of discount on short-term investments, net
(2,210)
(5,656)
(8,749)
(19,117)
Realized and unrealized loss (gain) on financial instruments, net
291
(338)
563
(1,190)
Unrealized foreign exchange loss (gain)
(171)
788
1,040
1,992
Change in operating assets and liabilities:
Accounts receivable, net
(66,993)
(24,557)
(25,188)
(11,258)
Prepaid expenses and other current assets
2,773
(1,964)
(1,883)
(582)
Deferred commissions
(3,548)
(18,821)
10,952
(38,794)
Other long-term assets
(2,931)
(8,395)
(13,999)
(17,704)
Accounts payable
4,993
1,370
3,555
1,569
Accrued liabilities
13,525
(6,719)
10,923
22,494
Operating lease liabilities
(3,570)
(3,777)
(8,321)
(9,145)
Deferred revenue
58,989
(17,039)
9,459
(71,352)
Other liabilities, non-current
730
92
(34)
(3,741)
Net cash provided by operating activities
143,510
37,438
325,544
99,653
Cash flows from investing activities
Purchases of property, equipment and other assets
(1,678)
(1,981)
(3,826)
(3,571)
Business combination, net of cash acquired
—
—
(2,032)
—
Investments in non-marketable securities
—
(250)
(8,322)
(5,750)
Proceeds from the sales of marketable securities
127,660
—
127,660
—
Proceeds from maturities of marketable securities
105,000
135,000
595,970
570,000
Purchases of marketable securities
—
(786,170)
(337,292)
(971,803)
Net cash provided by (used in) investing activities
230,982
(653,401)
372,158
(411,124)
Cash flows from financing activities
Repurchases of common stock
(148,633)
—
(343,079)
—
Proceeds from settlement of capped calls
—
—
—
170,589
Proceeds from the issuance of common stock under the Employee Stock Purchase Plan
—
—
22,917
18,640
Proceeds from exercise of stock options
533
315
2,322
1,621
Taxes paid related to net share settlement of equity awards
(38,496)
—
(38,496)
—
Principal payments of finance leases
(1,715)
(895)
(5,800)
(4,534)
Net cash (used in) provided by financing activities
(188,311)
(580)
(362,136)
186,316
Effect of exchange rate changes on cash, cash equivalents and restricted cash
783
(274)
8,851
(2,825)
Net increase in cash, cash equivalents and restricted cash
186,964
(616,817)
344,417
(127,980)
Cash, cash equivalents and restricted cash, beginning of period
650,206
1,292,480
492,753
803,643
Cash, cash equivalents and restricted cash, end of period
$ 837,170
$ 675,663
$ 837,170
$ 675,663
MONGODB, INC.
RECONCILIATION OF GAAP MEASURES TO NON-GAAP MEASURES
(in thousands of U.S. dollars, except share and per share data)
(unaudited)
Three Months Ended October 31,
Nine Months Ended October 31,
2025
2024
2025
2024
Reconciliation of GAAP gross profit to non-GAAP gross profit:
Gross profit on a GAAP basis
$ 449,132
$ 394,044
$ 1,260,079
$ 1,071,764
Gross margin (Gross profit/Total revenue) on a GAAP basis
71 %
74 %
71 %
74 %
Add back:
Expenses associated with stock-based compensation: Cost of Revenue—Subscription
9,230
7,999
26,752
22,145
Expenses associated with stock-based compensation: Cost of Revenue—Services
Reconciliation of GAAP operating expenses to non-GAAP operating expenses:
Sales and marketing operating expense on a GAAP basis
$ 230,864
$ 217,954
$ 695,852
$ 658,937
Less:
Expenses associated with stock-based compensation
38,579
42,155
116,172
125,129
Restructuring
251
—
4,775
—
Amortization of intangible assets
—
—
—
85
Non-GAAP sales and marketing operating expense
$ 192,034
$ 175,799
$ 574,905
$ 533,723
Research and development operating expense on a GAAP basis
$ 176,610
$ 151,410
$ 527,178
$ 446,437
Less:
Expenses associated with stock-based compensation
69,100
59,017
213,567
173,166
Restructuring
—
—
159
—
Amortization of intangible assets
170
170
510
2,908
Certain acquisition-related costs and other
—
—
40
—
Non-GAAP research and development operating expense
$ 107,340
$ 92,223
$ 312,902
$ 270,363
General and administrative operating expense on a GAAP basis
$ 60,082
$ 52,556
$ 174,321
$ 163,892
Less:
Expenses associated with stock-based compensation
16,396
16,377
48,452
50,469
Certain acquisition-related costs and other
4
—
1,894
—
Non-GAAP general and administrative operating expense
$ 43,682
$ 36,179
$ 123,975
$ 113,423
Reconciliation of GAAP loss from operations to non-GAAP income from operations:
Loss from operations on a GAAP basis
$ (18,424)
$ (27,876)
$ (137,272)
$ (197,502)
GAAP operating margin (Loss from operations/Total revenue)
(3) %
(5) %
(8) %
(14) %
Add back:
Expenses associated with stock-based compensation
138,090
129,186
418,752
381,303
Restructuring
250
—
5,022
—
Amortization of intangible assets
3,195
170
8,927
2,993
Certain acquisition-related costs and other
4
—
1,934
—
Non-GAAP income from operations
$ 123,115
$ 101,480
$ 297,363
$ 186,794
Non-GAAP operating margin (Non-GAAP income from operations/Total revenue)
20 %
19 %
17 %
13 %
Reconciliation of GAAP net loss to non-GAAP net income:
Net loss on a GAAP basis
$ (2,007)
$ (9,776)
$ (86,681)
$ (144,898)
Add back:
Expenses associated with stock-based compensation
138,090
129,186
418,752
381,303
Restructuring
250
—
5,022
—
Amortization of intangible assets
3,195
170
8,927
2,993
Certain acquisition-related costs and other
4
—
1,934
—
Amortization of debt issuance costs related to convertible senior notes
—
716
—
2,419
Less:
Gains (loss) on financial instruments, net
(291)
338
(563)
1,190
Income tax effects and adjustments *
25,279
21,858
60,434
40,809
Non-GAAP net income
$ 114,544
$ 98,100
$ 288,083
$ 199,818
Reconciliation of GAAP net loss per share, diluted, to non-GAAP net income per share, fully diluted:
Net loss per share, diluted, on a GAAP basis
$ (0.02)
$ (0.13)
$ (1.07)
$ (1.97)
Add back:
Expenses associated with stock-based compensation
1.70
1.75
5.15
5.19
Restructuring
—
—
0.06
—
Amortization of intangible assets
0.04
—
0.11
0.04
Certain acquisition-related costs and other
—
—
0.02
—
Amortization of debt issuance costs related to convertible senior notes
—
0.01
—
0.03
Less:
Gains (loss) on financial instruments, net
—
—
(0.01)
0.02
Income tax effects and adjustments *
0.31
0.30
0.74
0.56
Non-GAAP net income per share, diluted
$ 1.41
$ 1.33
$ 3.54
$ 2.71
Adjustment for fully diluted earnings per share
(0.09)
(0.17)
(0.22)
(0.32)
Non-GAAP net income per share, fully diluted **
$ 1.32
$ 1.16
$ 3.32
$ 2.39
* Non-GAAP financial information is adjusted for an assumed provision for income taxes based on our long-term projected tax rate of 20%. Due to the differences in the tax treatment of items excluded from non-GAAP earnings, our estimated tax rate on non-GAAP income may differ from our GAAP tax rate and from our actual tax liabilities.
** Fully diluted non-GAAP net income per share is calculated based upon 86.9 million and 86.8 million of fully diluted weighted- average shares of outstanding common stock for the three and nine months ended October 31, 2025, respectively, and 84.2 million and 83.7 million of fully diluted weighted-average shares of outstanding common stock for the three and nine months ended October 31, 2024, respectively.
The following table presents a reconciliation of free cash flow to net cash provided by operating activities, the most directly comparable GAAP measure, for each of the periods indicated (unaudited, in thousands):
Three Months Ended October 31,
Nine Months Ended October 31,
2025
2024
2025
2024
Net cash provided by operating activities
$ 143,510
$ 37,438
$ 325,544
$ 99,653
Capital expenditures
(1,678)
(1,981)
(3,826)
(3,571)
Principal payments of finance leases
(1,715)
(895)
(5,800)
(4,534)
Free cash flow
$ 140,117
$ 34,562
$ 315,918
$ 91,548
MONGODB, INC.
CUSTOMER COUNT METRICS
The following table presents certain customer count information as of the periods indicated:
10/31/2023
1/31/2024
4/30/2024
7/31/2024
10/31/2024
1/31/2025
4/30/2025
7/31/2025
10/31/2025
Total Customers(a)
46,400+
47,800+
49,200+
50,700+
52,600+
54,500+
57,100+
59,900+
62,500+
Direct Sales Customers(b)
6,900+
7,000+
7,100+
7,300+
7,400+
7,500+
7,500+
7,300+
7,000+
MongoDB Atlas Customers
44,900+
46,300+
47,700+
49,200+
51,100+
53,100+
55,800+
58,300+
60,800+
Customers over $100K(c)
1,972
2,052
2,137
2,189
2,314
2,396
2,506
5,564
2,694
(a) Our definition of “customer” excludes users of our free offerings and all affiliated entities are counted as a single customer.
(b) Direct Sales Customers are customers that were sold through our direct sales force and channel partners.
(c) Represents the number of customers with $100,000 or greater in annualized recurring revenue (“ARR”) and annualized monthly recurring revenue (“MRR”). ARR includes the revenue we expect to receive from our customers over the following 12 months based on contractual commitments and, in the case of Direct Sales Customers of MongoDB Atlas, by annualizing the prior 90 days of their actual consumption of MongoDB Atlas, assuming no increases or reductions in their subscriptions or usage. For all other customers of our self- serve products, we calculate annualized MRR by annualizing the prior 30 days of their actual consumption of such products, assuming no increases or reductions in usage. ARR and annualized MRR exclude professional services.
MONGODB, INC.
SUPPLEMENTAL REVENUE INFORMATION
The following table presents certain supplemental revenue information as of the periods indicated:
10/31/2023
1/31/2024
4/30/2024
7/31/2024
10/31/2024
1/31/2025
4/30/2025
7/31/2025
10/31/2025
MongoDB Enterprise Advanced: % of Subscription Revenue
27 %
26 %
25 %
24 %
25 %
23 %
22 %
21 %
20 %
Direct Sales Customers(a)
Revenue: % of Subscription Revenue
88 %
88 %
87 %
87 %
88 %
88 %
87 %
87 %
87 %
(a) Direct Sales Customers are customers that were sold through our direct sales force and channel partners.
Shares of Nvidia (NASDAQ:NVDA) edged about 1.5% higher on Monday morning after the company announced an expansion of their AI partnership.
The two firms will open an AI factory lab in Grenoble, France, designed to let customers test and refine AI workloads using HPE servers, networking, and Nvidia accelerated computing in a controlled, sovereign environment.
HPE also plans a Private AI Lab in London with Carbon3.ai and is expanding its HPE Unleash AI partner program, which now includes CrowdStrike (CRWD), to accelerate enterprise AI adoption in the U.K.
Executives said the labs will allow clients to validate performance, compliance, and data sovereignty before full-scale deployments, helping companies navigate regulatory hurdles and speed AI implementation.
The labs are part of HPE’s broader effort to provide turnkey AI factory stacks that simplify deployment across hybrid cloud and on-premises environments.
Analysts say the move could give enterprises a faster, safer path to scale AI operations globally while showcasing HPE and Nvidia’s combined infrastructure capabilities.
If you’re confused about the economy right now, you’re in good company. Experts are also grappling with conflicting indicators, imperfect data and flashing caution signs.
By some indicators, things seem to be going well. The stock market is up and rising. Unemployment – though ticking up – remains very low.
Yet by others, it could look like we’re heading for a downturn. Consumer sentiment is relatively low, consumer debt is high and stubborn inflation hasn’t budged much.
The state of the economy right now is “highly uncertain,” said Mark Gertler, economics professor at New York University. “It’s growing at a kind of modest growth rate, but there’s lots of uncertainty to play out.”
Put another way, nearly every metric economists use to determine the strength of the economy “is somewhere between moderately concerning” and “virtually stagnant,” added Ben Harris, vice president and director of Economic Studies at the Brookings Institution.
Add to that uncertainty the fact that key economic reports have been delayed or skipped over due to the record-breaking government shutdown, which ended last month.
Why does it matter that the overall picture is hazy? Complex data points make it tough for policy-makers to know the best course of action to help boost the economy, Gertler said. This is an especially complicated time for President Donald Trump’s administration, which is becoming the face of a worsening economy to many Americans. Affordability was a top issue for voters who overwhelmingly sent Democrats to power in the off-year elections in November.
Here are four important economic indicators, and what experts say they suggest about this moment.
1. The ‘no hiring, no firing’ labor landscape
The unemployment rate is still low, at around 4.4%, but has been steadily ticking up. Historically, employers need to add between 120,000 and 150,000 jobs per month to maintain a steady unemployment rate, Gertler said.
On Nov. 20, the Bureau of Labor Statistics released hiring numbers for September, delayed seven weeks due to the government shutdown. Though hiring had been weak since May, employers did pick up the pace in September, adding about 119,000 jobs.
One month doesn’t form a trend, Gertler said. A good jobs report helps make up some ground for four months of very low hiring, but overall the report was “neutral,” he said.
Right now, the labor market is in a “no hiring, no firing” position, Harris said. It’s tough to find a job if you don’t have one, but if you’re employed, you’re likely to keep that job. While that sounds stable, it’s actually a very precarious situation, he added.
“If employers start laying off workers, then you’re going to expand the supply of workers who could plausibly be hired. Then employers will feel more comfortable laying off workers because they know they can hire them if they need to,” he said.
Though different economists might have varying views on whether the market will steady or deteriorate, Harris said he doesn’t know of “any labor market optimists right now.”
“Once the layoffs start,” he added, “they could come fast and furious.”
When it comes to interpreting the numbers, Trump’s immigration policy is a key variable. The unemployment rate is the number of people who are unemployed divided by the number of people in the labor force. But that denominator is shrinking with the Trump’s administration’s aggressive deportation policy, said Joanne Hsu, director of the Surveys of Consumers at the University of Michigan. And a smaller supply of workers could lead employers to hire less, Gertler said.
Other factors that could be affecting hiring include the rise of artificial intelligence, which could be displacing human jobs, or just a generally weak economy.
WATCH: 3 things to know about AI and mass corporate layoffs
It’s unclear if the weak job market is caused by low labor supply or low hiring demand, Gertler said.
“It’s not as dire a situation as during the great financial crisis [of 2008], but in some ways it’s more complex because it’s hard to know which direction to go,” Gertler said. “During the great financial crisis, you knew the policy should be: you have expansionary monetary policy and fiscal policy. Here, it’s really tough to say.”
2. The lower inflation trade-off
One metric that’s dominated headlines since 2021 is the consumer price index, which measures change in prices over time, also known as inflation.
Between Sept. 2024 and Sept. 2025, the core CPI, which tracks all consumer prices excluding food and energy, increased 3%. That’s down from a high of 6.6% in Sept. 2022, but still above the government’s target rate of around 2% – a number not seen since early 2021.
Any movement toward that 2% goal would be a sign in the right direction, Gertler said. But inflation below that could also indicate a weakening economy.
For almost five years now, the Federal Reserve has been trying to tame inflation, and has only just begun lowering interest rates. A weak economy will see softening inflation, which could also reflect a slowing job market, as we’ve been experiencing.
READ MORE: The Federal Reserve wrestles with how many interest rate cuts to make and how fast
That’s the kind of trade-off the Federal Reserve might have to make, Gertler said.
“It may be some slowing of the economy is required to get the inflation rate down, but this is why the Fed is going gradually, so that it won’t have to be too disruptive to the labor market,” he said.
Harris also said that massive shortages in the housing market have been a major contributor to inflation since 2023. Housing alone takes up about a third of the CPI, according to Brookings.
“If housing inflation is 5 or 6%, it’s really, really hard to get down to 2% inflation,” Harris said.
In that case, the Fed raising interest rates – their typical response to rising inflation – won’t really help, he said. It might discourage more people from taking out loans to buy housing, but it also means more people won’t be selling, which reduces supply, he said.
3. A ‘flashing yellow light’ of consumer debt
Consumer debt in the U.S. is at an all-time high, with Americans owing $18.59 trillion, according to the Federal Reserve Bank of New York’s latest report. That debt includes student loans, auto loans, mortgages, home equity lines of credit, credit card debt and other loans.
When considering consumer debt, it’s important to break down macro and micro interpretations, Harris said.
On the whole, “consumption is really strong in the United States, and has always driven our economy – and it’s no different today,” Harris said.
READ MORE: Despite economic uncertainty, Cyber Monday could break spending records
Current debt payments as a percentage of personal income are relatively low, historically speaking. Debt payments comprise about 11% of personal income across all U.S. households, far lower than the almost 16% high it hit during the Great Recession and slightly lower than before the pandemic.
It’s one example of an economic indicator that may look unconcerning on the surface. However, Hsu said, looking at aggregate data alone may obscure worse or better factors in specific parts of the economy.
“On aggregate, things can look fine, and that would be totally consistent with vulnerabilities showing up, because the aggregate numbers are not good at identifying specific vulnerabilities,” she said.
One way to look under the hood is to examine transitions into delinquency. Credit card and consumer loan delinquency both began steadily rising in 2021, though there are signs they’ve leveled off.
“We’re not yet seeing foreclosures tick up very much, and so this is not necessarily 2008 all over again. The worst type of transitions into delinquency are when people can’t make payments on their home. It’s one thing to not be able to make a payment on your credit card; it’s another thing to worry about getting evicted,” Harris said, adding that he sees this moment as more of a “flashing yellow light, not a flashing red light.”
4. A self-fulfilling consumer sentiment prophecy?
In November, the University of Michigan’s Index of Consumer Sentiment fell to 51, down from nearly 72 a year ago.
That decrease is driven by twin pressures, said Hsu, the survey’s director. At the same time that consumers are frustrated by high prices, they’re also worried about the stability of their incomes.
READ MORE: How to make the most of your holiday gift budget
The second worry in particular defines this period of low sentiment, she said, unlike in the inflationary period right after the pandemic.
“We still have people who are unhappy about high prices, cost of living, affordability. But unlike three years ago, now they’re also worried about their incomes,” Hsu said.
She added that when they asked people if they think unemployment will get worse in the year ahead, 69% said yes, more than double the number of people who felt that way last November.
Breaking down respondents into higher- and lower-income households can also help clarify how people view the economy right now.
“The lion’s share of consumer spending is being generated by higher-income and higher-wealth consumers,” Hsu said. Those people still “don’t feel great” about the economy right now either, but they’re backed by strong financial assets, stock values and incomes, so they report they feel supported to keep spending. Middle- and lower-income people are much less likely to report that they expect their income to increase next year compared to higher-income individuals.
Consumer sentiment can also align along partisan lines. Michigan’s data, which include respondents’ political parties, show that the overall national results track closely with how independent voters feel.
Though consumer sentiment might seem more reflective than predictive, there’s the possibility that it could become a self-fulfilling prophecy, Hsu said.
“It’s called ‘the paradox of thrift,’ where if you think dark times are ahead, it makes sense for each individual family to pull back, to save more, to save for the rainy day and protect themselves. But if enough people do that, people are going to stop spending on a large scale,” she said.
The result could be businesses losing money, laying off workers and ultimately generating a negative feedback loop.
A free press is a cornerstone of a healthy democracy.
Editors’ Highlights are summaries of recent papers by AGU’s journal editors.
Source: AGU Advances
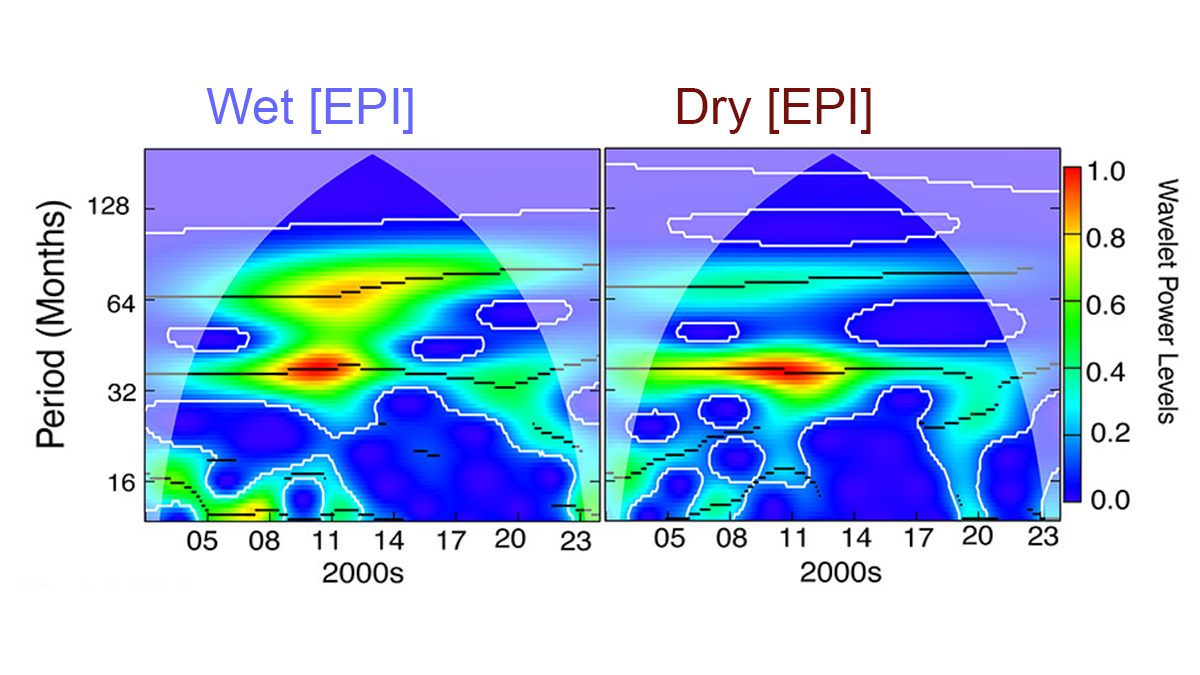
Using data from the GRACE and GRACE-FO satellite missions, Rateb et al. [2025] monitored global changes in terrestrial water storage to study how hydrological extremes—floods and droughts—have developed over the past two decades. Their analysis indicates that these extremes are mainly driven by climate variability in tropical oceans, with both interannual and multi-year patterns playing a significant role.
However, the approximately 22-year satellite record is still too short to fully identify long-term drivers, which limits the ability to determine whether global extremes are increasing or decreasing. To fill data gaps in certain months, the authors use non-parametric probabilistic methods to reconstruct storage anomalies. The reconstructed data closely matched independent datasets, confirming the reliability of their approach. Overall, the study highlights the need to extend satellite observations to capture multi-decadal climate variability and better distinguish natural fluctuations from human-induced changes.
Citation: Rateb, A., Scanlon, B. R., Pokhrel, Y., & Sun, A. (2025). Dynamics and couplings of terrestrial water storage extremes from GRACE and GRACE-FO missions during 2002–2024. AGU Advances, 6, e2025AV001684. https://doi.org/10.1029/2025AV001684
Sleep disorders are a significant public health concern, with about two-thirds of adults worldwide reporting at least one sleep-related problem []. Their prevalence has been confirmed not only among the general adult population [] but also in specific groups such as nursing students [] and cancer survivors []. The consequences extend beyond physical health, as poor sleep has been consistently linked to adverse mental health outcomes [] and overall diminished well-being []. Conditions such as insomnia, sleep apnea, and restless legs syndrome affect individuals across different age groups, significantly reducing quality of life []. While severe cases may require medical treatment, early intervention through lifestyle adjustments and access to reliable information is crucial for mitigating symptoms in their initial stages []. If left unaddressed, the chronic nature of sleep disorders can result in long-term health problems, underscoring the need for accessible and trustworthy health information.
As many individuals are unaware of the early signs of these conditions, they often turn to the internet for information, which may not always be accurate or trustworthy []. This points to the importance of eHealth literacy—the ability to find, understand, and apply reliable health information found online []. eHealth literacy has been conceptualized as a multidimensional construct extending traditional notions of health literacy to the digital environment, encompassing skills to navigate, evaluate, and use online health resources effectively []. However, individuals seeking health information online encounter challenges such as information overload [] and exposure to health misinformation [], highlighting why eHealth literacy remains crucial for the effective use of online health resources [].
The most widely used instrument, eHealth Literacy Scale (eHEALS), is based on self-reports and does not cover functional, communicative, or critical skills []. To address these limitations, alternative instruments have been developed, such as the Transactional Model of eHealth Literacy, which outlines functional, communicative, critical, and translational dimensions of eHealth literacy [], and the CoV-eHEALS, which was validated during the COVID-19 pandemic but also revealed the tendency of self-reports to overestimate actual ability []. Nevertheless, most studies continue to rely on self-reported measures, leaving the link between perceived ability and actual knowledge uncertain []. Reviews have emphasized the importance of examining how eHealth literacy relates to objective knowledge outcomes [].
Search frequency has been shown to exert an independent influence on knowledge acquisition. On the one hand, more frequent searching can increase awareness and exposure to health information [,]. On the other hand, it may also lead to information overload and conflicting messages, which can reduce factual accuracy [,]. This dual nature suggests that search frequency itself functions as a predictor of knowledge outcomes, beyond the role of eHealth literacy. Prior research also indicates that eHealth literacy predicts positive health behaviors even after controlling for search frequency [], underscoring the importance of considering search frequency and literacy as distinct explanatory factors.
In addition, information-seeking behaviors may influence how eHealth literacy translates into knowledge. While prior work has typically examined literacy and information seeking as separate predictors [] or emphasized their independent contributions [], less attention has been paid to their potential interaction. This gap highlights the need to examine whether the effect of eHealth literacy on knowledge varies depending on search frequency. In the context of sleep disorders, where accurate knowledge is essential but often limited, such an interplay may be particularly consequential.
Research on other conditions supports this view. eHealth literacy has been linked to knowledge in chronic obstructive pulmonary disease [], colorectal cancer [], and COVID-19 []. However, such evidence is scarce in the context of sleep. The concept of sleep health literacy emphasizes the competencies required to recognize and manage sleep problems []. Building on this, recent studies have introduced validated measurement tools for sleep health literacy []. Yet, awareness of sleep disorders remains low even among medical professionals [], and education has been shown to improve knowledge without necessarily enhancing sleep quality []. These observations indicate that knowledge about sleep disorders is both important and underexplored. Thus, there is a need to examine both the independent and combined effects of eHealth literacy and search frequency in shaping sleep disorder knowledge.
Objectives
This study addresses this gap by examining how eHealth literacy and search frequency jointly influence objective knowledge about sleep disorders. By testing both their independent and interactive contributions, the study extends prior work that has typically considered these factors in isolation, situating the analysis in the understudied context of sleep disorders. illustrates the hypothesized research model.
Figure 1. Hypothesized research model.
Our hypotheses were as follows:
H1: eHealth literacy will be positively associated with objective knowledge about sleep disorders.
H2: Search frequency will be positively associated with objective knowledge about sleep disorders.
H3: The association between eHealth literacy and objective knowledge will be moderated by the frequency of health information searches.
H2: Search frequency will be positively associated with objective knowledge about sleep disorders.
H3: The association between eHealth literacy and objective knowledge will be moderated by the frequency of health information searches.
Methods
Participants
The study employed a cross-sectional online survey design and initially recruited 280 participants from psychology classes at Ulm University in Ulm, Germany, using a convenience sampling approach. Eligibility criteria required participants to be at least 18 years old and proficient in the German language. After excluding 14 participants, the data from 266 respondents were used for analysis. Specifically, 9 participants were excluded because they were not fluent in German, and 5 participants were excluded for not completing the survey in a serious manner, as indicated by inconsistent or patterned responses. A sensitivity power analysis using G*Power (F tests, multiple regression: R2 increase; α=.05, 1–β=.80, 1 tested predictor, total predictors=7) indicated that with 266 participants, the study was sufficiently powered to detect a small incremental effect (f2=0.03).
Ethical Considerations
The study was reviewed by the ethics committee of Ulm University, which determined that detailed ethical approval was not necessary. Participation was voluntary, and all respondents provided informed consent before beginning the survey. Data were collected anonymously through an online survey tool (Survey Coder Tool by Christopher Kannen []), and no personally identifying information was retained. Participants received course credit as compensation for their involvement. Participants were also informed that their anonymized data could be shared for research purposes following publication. The study design and reporting followed the CHERRIES (Checklist for Reporting Results of Internet E-Surveys; ).
Measurements
eHealth Literacy
The level of eHealth literacy was assessed using the revised eHEALS. This scale is based on the original eHEALS items developed by Norman and Skinner [], with additional items from the eHEALS-E questionnaire []. The German version of the scale was applied (see ), with all items translated into German (2 independent bilingual scientists performed a back-and-forth translation). The eHEALS consists of 8 questions, each rated on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree), with a total score ranging from 8 to 40, measuring participants’ perceived eHealth literacy. The validity of the revised version of eHEALS was confirmed through a confirmatory factor analysis. The analysis of the 8-item model indicated a good fit for the proposed model (χ27=4.728, P=.693, comparative fit index=1.000, Tucker-Lewis index=1.000, root mean square error of approximation=0.000, standardized root mean square residual=0.013). The internal consistency of the test was confirmed using McDonald’s omega coefficient (ω=0.854). The specific items of this eHEALS were as follows:
I know how to find helpful health information on the internet.
I know how to use the internet to answer my health questions.
I know what health resources are available on the internet.
I know where to find helpful health resources on the internet.
I know how to use the health information I find on the internet to help me.
I have the skills I need to evaluate the health resources I find on the internet.
I can tell high-quality from low-quality health resources on the internet.
I feel confident in using information from the internet to make health decisions.
Objective Knowledge Regarding Sleep Disorders
Objective knowledge about sleep disorders was measured using a 15-item scale, adapted from a previous study []. A total of 15 items were initially measured on a 7-point scale (1=Sure this is incorrect, 7=Sure this is correct) and later dichotomized into correct (1) and incorrect (0) responses for hypothesis testing. The German version of the scale was applied (see ), with all items translated into German (again, 2 bilingual scientists performed the back-and-forth translation process, see above). The specific items are listed below, with the correct answers indicated in parentheses (T=true, F=false). The total score ranged from 0 to 15, with higher scores reflecting greater factual knowledge of sleep disorders.
Drinking 3 standard glasses of alcohol has no effect on sleep. (F)
Taking a prescription sleep medication can cause stomach problems like nausea and gas. (T)
Smoking more than 1 pack of cigarettes a day has no effect on sleep. (F)
Leaving a light on benefits sleep. (F)
Going to bed thirsty has an effect on sleep. (T)
If you cannot fall asleep in 20 minutes, you should get out of bed and try again later. (T)
Prescription sleep medications are designed to be taken for a long period of time. (F)
Going to bed at the same time each night disrupts sleep. (F)
You should spend 2 hours longer in bed than you need for sleep to give yourself the best opportunity. (F)
Consuming food, beverages, or medications containing caffeine has no effect on sleep. (F)
Regular exercise at least 4 hours before going to bed benefits sleep. (T)
Prescription sleep medications should be taken just before going to bed. (T)
If you wake during the night and cannot fall back to sleep within 20 min, you should stay in bed and try harder. (F)
Stress and anxiety can make it harder to fall asleep but do not affect the length of sleep. (F)
Newer prescription sleep medications (nonbenzodiazepines) are safer because they do not lead to dependence. (F)
Frequency of Internet Searching
The frequency of internet searches for health information was assessed based on the daily number of searches conducted by the participants. This frequency was measured using a single-item scale (also presented in the German language). Respondents indicated their agreement with the following statements: “Have you searched on the internet for information on your health, health problems, or medical treatments in the last 6 months? (Haben Sie in den letzten sechs Monaten im Internet nach Informationen zu Ihrer Gesundheit, Gesundheitsproblemen oder medizinischen Behandlungen gesucht?)” The item was measured on a 3-point Likert scale (1=None, 2=1 or 2 times, 3=More than twice). Previous studies have identified a positive association between eHealth literacy and the frequency of internet searches [,]. Based on the previous studies, in this study, we used the frequency of internet searching as a moderating variable to examine how it influences the relationship between eHealth literacy and objective knowledge about sleep disorders.
Covariates
In addition to the above endogenous variables, we also controlled for our participants’ age, gender, education level, and past experience with sleep disorders as exogenous variables to make sure that the sample represents the population.
Statistical Analysis
To test H1 and H2, hierarchical multiple regression analysis was conducted with objective knowledge as the dependent variable. In step 1, demographic variables (age, gender, and education) were entered as controls. In step 2, past experience with sleep disorders was added. In step 3, eHealth literacy was included, and in step 4, search frequency was added. Continuous predictors were mean-centered prior to these regression analyses. To test H3, the interaction between eHealth literacy and search frequency was examined using the PROCESS macro for SPSS (model 1; Hayes []) with 5000 bootstrap samples []. This approach estimated the conditional effects of eHealth literacy on knowledge at different levels of search frequency. All analyses were performed with SPSS Statistics (version 26; IBM Corp.).
Results
Validation of the Objective Knowledge Regarding Sleep Disorders
To evaluate the properties of the adapted sleep knowledge scale, item- and scale-level analyses were conducted. Item-total correlations were generally low, which is expected in factual knowledge tests because each item represents an independent piece of information. Sampling adequacy was acceptable (Kaiser-Meyer-Olkin=0.667), and Bartlett test indicated that the correlation matrix was factorable (χ2105=369.25; P<.001). An exploratory factor analysis using principal axis factoring with oblimin rotation suggested limited unidimensionality: although 6 components had eigenvalues greater than 1 (first eigenvalue=2.59), the first extracted factor explained only 13.14% of the variance, and item loadings were widely dispersed. Internal consistency based on a single-factor model was also low (ω=0.20), consistent with the expectation that the scale functions as an index of heterogeneous factual knowledge rather than a unidimensional construct.
Evidence for validity was supported by positive correlations of the knowledge score with eHealth literacy (r=0.30; P<.001) and with recent general online health information seeking (r=0.27; P<.001). In contrast, neither sleep problem experience (r=−0.03; P=.67) nor sleep-specific information seeking (r=−0.01; P=.89) was significantly related to knowledge.
Known-groups validity was further supported by higher knowledge scores among participants who had searched for health information in the past 6 months compared with those who had not (mean difference=1.27, P=.004 for none vs once or twice; mean difference=1.84, P<.001 for none vs more than twice; Bonferroni-adjusted). No significant group differences were observed for sleep problem experience (F3,262=0.78; P=.50) or for sleep-specific searches (F2,263=2.10; P=.13). Taken together, these findings indicate that the adapted scale captures factual accuracy across diverse content areas and is appropriate for use as a knowledge index in this study.
Sample Characteristics
The study sample consisted of 266 participants, of whom 229 (86.1%) were female and 37 (13.9%) were male. The mean age of the respondents was 21.78 (SD 3.35; range 18‐52) years. Most (n=217, 81.6%) participants were in the 20‐29 years age range. A smaller proportion (n=42, 15.8%) were younger than 20 years, 2.4% (n=6) were aged 30‐39 years, and 0.4% (n=1) were 40 years and older. Regarding educational attainment, the majority (n=242, 91.0%) held a high school diploma. Other levels included intermediate technical qualifications (n=4, 1.5%), University of Applied Sciences degrees (n=3, 1.1%), and university degrees (n=16, 6.0%). Only 1 (0.4%) participant reported a secondary school leaving certificate. All participants were native German speakers (n=266, 100%). These demographic characteristics are summarized in .
Table 1. Participants’ demographics (N=266).
Characteristic
Participants, n (%)
Gender
Male
37 (13.9)
Female
229 (86.1)
Age (y)
<20
42 (15.8)
20‐29
217 (81.6)
30‐39
6 (2.4)
≥40
1 (0.4)
Education achievement
Secondary school leaving certificate
1 (0.4)
Intermediate technical qualification
4 (1.5)
High school diploma
242 (91)
University of applied sciences degree
3 (1.1)
University degree
16 (6)
Native German
Yes
266 (100)
No
0 (0)
Prior to analyzing the hypothesized model, descriptive statistics and Pearson correlations were computed ().
Table 2. Means, standard deviations, and correlations of all variables.
1
2
3
4
5
6
7
Age
1
Gender
−0.10
1
Education
0.14
0.04
1
Past experience
0.03
0.04
0.05
1
eHealth literacy
0.07
−0.02
0.06
−0.04
1
Search frequency
−0.03
0.04
0.04
0.02
0.08
1
Objective knowledge
−0.02
0.02
0.09
−0.03
0.30
0.27
1
Mean (SD)
21.78 (3.35)
1.86 (.35)
5.11 (.52)
2.50 (.99)
3.68 (.64)
2.32 (.70)
11.24 (2.14)
aValues are Pearson correlation coefficients. Correlations of age with education (r=0.14; P=.02), eHealth literacy with objective knowledge (r=0.30; P<.001), and search frequency with objective knowledge (r=0.27; P<.001) were significant; all other correlations were nonsignificant.
bNumbers (1-7) refer to the variable labels listed in the leftmost column (Age to Objective knowledge).
Main Association Analysis
To test H1 and H2, we conducted hierarchical multiple regression analyses with objective knowledge as the dependent variable. summarizes the results.
Table 3. Results of hierarchical multiple regression analyses on objective knowledge (N=266).
Objective knowledge
B
SE
ß
t test (df)
P value
Step 1
Age
–0.03
0.06
–0.03
–0.49 (262)
.62
Gender
–0.01
0.06
–0.01
–0.14 (262)
.89
Education
0.09
0.06
0.09
1.47 (262)
.14
Step 2
Age (y)
–0.03
0.06
–0.03
–0.48 (261)
.63
Gender
–0.01
0.06
–0.01
–0.15 (261)
.88
Education
0.09
0.06
0.09
1.49 (261)
.14
Past experience
–0.03
0.06
–0.03
–0.49 (261)
.63
Step 3
Age
–0.05
0.06
–0.05
–0.78 (260)
.44
Gender
–0.01
0.06
–0.01
–0.23 (260)
.82
Education
0.07
0.06
0.08
1.28 (260)
.20
Past experience
–0.02
0.06
–0.02
–0.29 (260)
.77
eHealth literacy
0.29
0.06
0.30
4.97 (260)
<.001
Step 4
Age
–0.04
0.06
–0.04
–0.63 (259)
—
Gender
–0.01
0.06
–0.01
–0.08 (259)
—
Education
0.07
0.06
0.06
1.16 (259)
—
Past experience
–0.02
0.06
–0.02
–0.39 (259)
—
eHealth literacy
0.27
0.06
0.27
4.75 (259)
<.001
Search frequency
0.24
0.06
0.24
4.20 (259)
<.001
aGender coded as female=0, male=1. ΔR2 values correspond to variance explained by each step.
bB: unstandardized coefficient.
cβ: standardized coefficient.
dModel summary: P=.51; F3,262=0.768; ΔR2=0.009.
eModel summary: P=.64; F4,261=0.634; ΔR2=0.001.
fModel summary: P<.001; F5,260=5.488; ΔR2=0.086.
gModel summary: P<.001; F6,259=7.801; ΔR2=0.058.
hNot applicable.
In step 1, demographic variables including age, gender, and education were entered into the model. Age, gender, and education were not significant predictors of objective knowledge. This model accounted for 0.9% of the variance (ΔR2=0.009; F3,262=0.768; P=.51).
In step 2, past experience with sleep disorders was added, but it did not significantly predict objective knowledge. This step explained an additional 0.1% of the variance (ΔR2=0.001; F4,261=0.634; P=.64).
In step 3, we added eHealth literacy to the model. eHealth literacy emerged as a significant predictor (B=0.29, SE 0.06; t260=4.97; P<.001), explaining an additional 8.6% of the variance (ΔR2=0.086; F5,260=5.488; P<.001). Higher eHealth literacy was associated with greater objective knowledge. However, age, gender, education, and past experience were nonsignificant.
In step 4, the search frequency was entered. Search frequency emerged as an additional significant predictor (B=0.24, SE 0.06; t259=4.20; P<.001), accounting for an additional 5.8% of the variance (ΔR2=0.058; F6,259=7.801; P<.001). The overall model explained 15.3% of the variance (R2=0.153).
In sum, these findings indicate that eHealth literacy and search frequency both contribute significantly to objective knowledge about sleep disorders, even after accounting for demographic factors and past experience with sleep disorders.
Moderation Analysis
The main effect of eHealth literacy on objective knowledge about sleep disorders was significant, with higher eHealth literacy predicting greater knowledge (B=2.33, SE 0.66; t259=3.56; P<.001; 95% CI 1.04-3.62; see ). Similarly, more frequent health information searches were associated with higher objective knowledge (B=3.00, SE 1.02; t259=2.94; P=.004; 95% CI 0.99-5.00). The interaction between eHealth literacy and health information search frequency was also significant (B=−0.61, SE 0.27; t259=−2.24; P=.03; 95% CI −1.15 to −0.07), indicating a moderation effect.
Table 4. Moderated effect: search frequency as a moderator in the association between eHealth literacy and objective knowledge (N=266).
Predictor
B
SE
t test (df)
P value
95% CI
eHealth literacy
2.33
0.66
3.56 (259)
<.001
1.04 to 3.62
Search frequency
3.00
1.02
2.94 (259)
.004
0.99 to 5.00
eHealth literacy × search frequency
–0.61
0.27
–2.24 (259)
.03
–1.15 to –0.07
aCovariates (age, gender, and past experience with sleep disorders) were included in the model.
bModel summary: R2=0.165; F6,259=8.52; P<.001.
Conditional effects showed that when search frequency was low (−1 SD), the positive effect of eHealth literacy on knowledge was strong (B=1.35, SE 0.27; t259=5.04; P<.001; 95% CI 0.82 to 1.87). At the mean level of search frequency, the effect remained significant but weaker (B=0.92, SE 0.19; t259=4.80; P<.001; 95% CI 0.54-1.30). At the highest observed level of search frequency, the effect was no longer significant (B=0.50, SE 0.27; t259=1.86; P=.06; 95% CI −0.03 to 1.03). These findings indicate that the contribution of eHealth literacy to knowledge acquisition depends on search frequency, with the effect attenuating as search frequency increases. The overall model was significant (R2=0.165; F6,259=8.52; P<.001). These conditional effects are summarized in .
Table 5. Conditional effects of eHealth literacy on objective knowledge at values of search frequency.
Search frequency level
B
SE
t test (df)
P value
95% CI
Low (–1 SD)
1.35
0.27
5.04 (259)
<.001
0.82 to 1.87
Mean
0.92
0.19
4.80 (259)
<.001
0.54 to 1.30
High (maximum observed)
0.50
0.27
1.86 (259)
.06
–0.03 to 1.03
aConditional effects estimated with PROCESS Model 1 (5000 bootstrap samples).
These results are illustrated in , which depicts the interaction effects between eHealth literacy and health information search frequency on objective knowledge.
Figure 2. Objective knowledge as a function of eHealth literacy and search frequency.
Discussion
Principal Results
This study investigated how eHealth literacy and the frequency of health information searches contribute to knowledge about sleep disorders. The results indicated positive main effects of both eHealth literacy (H1) and search frequency (H2), as well as a moderation effect showing that the contribution of literacy was conditioned by search frequency (H3).
Comparison With Previous Work
Consistent with H1, higher eHealth literacy was positively associated with greater knowledge about sleep disorders. Prior research has shown that literacy enhances the ability to evaluate online health information accurately [] and contributes to more reliable knowledge in disease-specific contexts such as COVID-19 []. Similar associations have also been reported in colorectal cancer [,].
In line with H2, search frequency itself was positively associated with knowledge outcomes. Studies have indicated that active searching increases awareness and factual accuracy [,]. At the same time, frequent searching can expose individuals to information overload or conflicting messages, which may reduce accuracy [,]. These findings suggest that the effects of search frequency are not uniform across contexts.
Most importantly, H3 was supported. The positive association between eHealth literacy and knowledge was the strongest when search frequency was low, whereas the effect diminished and became nonsignificant at higher levels of searching. This pattern demonstrates that eHealth literacy and information-seeking behavior interact to determine knowledge outcomes rather than exerting independent effects. Previous studies, however, have primarily examined the independent effects of literacy [] or of search behavior [,], without considering how they may interact. Our findings highlight that treating literacy and search in isolation may overlook the ways in which cognitive capacities and behavioral patterns jointly shape knowledge outcomes. The observed attenuation of literacy’s effect at higher search frequencies may be explained by multiple mechanisms, including information overload that reduces the marginal value of repeated searching [] and variability in the quality of retrieved information []. Together, these results underscore that eHealth literacy and information-seeking behavior are interdependent factors that jointly shape how effectively individuals acquire accurate health knowledge.
Finally, this study extends eHealth literacy research to the underexplored context of sleep disorders. Few studies have examined sleep-specific knowledge in relation to literacy [,]. Intervention studies have also yielded mixed outcomes, with awareness and knowledge improving but effects on sleep quality being less consistent []. By developing and validating a new measure of objective knowledge about sleep disorders, this study addresses this gap and provides a methodological contribution to advancing sleep health literacy research.
Limitations, Implications, and Future Directions
Beyond these findings, several limitations should be acknowledged. First, the sample size, while sufficient for the analyses conducted, may limit the generalizability of the findings. The sample was heavily skewed toward young, female psychology students (N=266; mean age=21.78, SD 3.35; n=229, 86.1% female), which constrains external validity. Prior studies have shown that eHealth literacy and information processing can vary across age [] and education levels [,], suggesting that the present findings may not generalize to broader populations. The restricted age variance may also help explain why demographic effects, such as age, were not significant in this study. Future research should seek to include a larger, more diverse population to strengthen the external validity of these results.
Second, while this study successfully demonstrated the association between eHealth literacy and actual knowledge levels, it did not account for the outcomes resulting from actual behavior. Future research should examine whether and how these search activities lead to increased knowledge, and more importantly, how these processes occur. This could involve investigating the quality of information accessed, the strategies used to evaluate and apply this information, and the extent to which these factors contribute to knowledge acquisition and behavior change.
Third, the study highlighted the interaction pattern of search behavior on the relationship between eHealth literacy and objective knowledge. However, it did not delve into the underlying causes of this search behavior. Future research should consider various factors related to media search behavior, such as motivation, accessibility, and past experiences, to better understand the background of these actions. By exploring these variables, researchers can gain insights into what drives individuals to engage in frequent health information searches and how these behaviors interact with eHealth literacy to influence knowledge outcomes.
Lastly, the measure of health information search frequency was self-reported, which introduces potential biases in reporting. Participants may overestimate or underestimate their search behavior, which could influence the accuracy of the results. Objective measures of search behavior, such as tracking actual online searches, would provide a more precise understanding of how frequently individuals seek out health information and how that correlates with knowledge acquisition.
Beyond methodological limitations, the findings also carry theoretical and practical implications. Theoretically, this study contributes to eHealth literacy research by clarifying that the effect of literacy is most evident when search frequency is low, and by demonstrating the value of integrating a behavioral factor as a moderator. It also offers a methodological contribution through the development of a disease-specific objective knowledge scale for sleep disorders. This scale can serve as a useful tool for evaluating the outcomes of literacy-based interventions and for assessing knowledge of sleep disorders in future research. Practically, the results point to the value of strengthening literacy among individuals who search less frequently, while digital platforms may support low-literacy users by embedding credibility cues or sleep-education modules. Taken together, these insights suggest that literacy enhancement efforts should be accompanied by training on critical information management, which can inform digital health education and patient-support initiatives. Such strategies can provide useful guidance for educators, clinicians, and public health agencies seeking to improve sleep-related health knowledge.
Conclusion
This study examined how eHealth literacy and health information seeking jointly influence knowledge acquisition. We found that higher eHealth literacy was associated with greater sleep disorder knowledge, and more frequent health information searches were also positively related to knowledge. However, the effect of eHealth literacy was varied by search frequency. The positive association was evident among individuals who searched less often, but it diminished at higher levels of search activity. These findings highlight that the role of eHealth literacy is not uniform and depends on behavioral patterns of information seeking. Understanding this interaction clarifies how cognitive capacities and behaviors jointly influence knowledge acquisition and has implications for digital health education, suggesting that literacy support may be more effective when combined with strategies for managing online information. Overall, the study contributes by clarifying the conditions under which eHealth literacy exerts its strongest effects and by extending research to the context of sleep disorders with a newly developed objective knowledge scale. This scale can be used to assess knowledge of sleep disorders and to guide literacy-based health education.
This work was supported by the 2025 Korean Studies Grant Program of the Academy of Korean Studies (AKS-2025-E-004). The authors acknowledge the use of a generative artificial intelligence tool (ChatGPT, OpenAI) to assist only with language editing of certain passages; all content was created and verified by the authors.
This work was supported by the 2025 Korean Studies Grant Program of the Academy of Korean Studies (AKS-2025-E-004).
The datasets generated and analyzed during this study are available from the corresponding author upon reasonable request.
None declared.
Edited by Amy Schwartz; submitted 03.Dec.2024; peer-reviewed by Basil Alzougool, Ramya Kr; final revised version received 17.Oct.2025; accepted 31.Oct.2025; published 01.Dec.2025.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work, first published in the Journal of Medical Internet Research (ISSN 1438-8871), is properly cited. The complete bibliographic information, a link to the original publication on https://www.jmir.org/, as well as this copyright and license information must be included.
The European Commission has approved the subcutaneous administration route and pharmaceutical form of pembrolizumab (pembrolizumab and berahyaluronidase alfa; Keytruda SC) for all adult indications of the intravenous (IV) form of pembrolizumab (Keytruda) in the European Union.1
Comparable efficacy results with subcutaneous pembrolizumab vs IV pembrolizumab in patients with metastatic non–small cell lung cancer (NSCLC) from the phase 3 3475A-D77 trial (NCT05722015) informed the European Commission’s decision. The primary analysis of the trial solidified subcutaneous administration of pembrolizumab (n = 251) as noninferior to pembrolizumab IV (n = 126), with the overall response rate (ORR) in the subcutaneous pembrolizumab arm being 45% (95% Cl, 39%-52%) vs 42% (95% Cl, 33%-51%) in the pembrolizumab IV arm.1,2 Efficacy results for progression-free survival (PFS) and overall survival (OS) had no differences between patients in each arm of the trial. Furthermore, the geometric mean ratio (GMR) for cycle 1 at AUC0-6 weeks was 1.14 (96% CI, 1.06-1.22; P < .0001), and the GMR for steady-state Ctrough was 1.67 (94% CI, 1.52-1.84; P < .0001).2
“We are honored to introduce [subcutaneous pembrolizumab], the first and only subcutaneous immune checkpoint inhibitor in Europe that can be administered in 1 minute every 3 weeks or in 2 minutes every 6 weeks,” Marjorie Green, MD, senior vice president and head of Oncology and Global Clinical Development at Merck Research Laboratories, stated in a news release.1 “We are committed to discovering patient-focused innovations for people with cancer, like [subcutaneous pembrolizumab], which offers faster administration than [IV pembrolizumab], 2 dosing options, and allows patients more choices of health care settings where they can receive therapy.”
The subcutaneous method of administration implements medications under the skin, enabling administration times that can be as little as 1 minute. The technology offers convenience to patients since they can receive medications through subcutaneous administration in a larger range of settings like community clinics, rather than purely at infusion centers. Moreover, subcutaneous administration offers patients whose veins are hard to access for IV infusion a more accessible method of receiving treatment.
Subcutaneous Pembrolizumab Approved in EU for All Adult Indications: Key Takeaways
The European Commission has approved the subcutaneous administration route and pharmaceutical form of pembrolizumab for all adult indications of the IV form in the European Union.
In the phase 3 3475A-D77 trial (NCT05722015) subcutaneous administration of pembrolizumab was noninferior to pembrolizumab IV, with an ORR in the subcutaneous pembrolizumab arm of 45% (95% Cl, 39%-52%) vs 42% (95% Cl, 33%-51%) in the pembrolizumab IV arm.
Subcutaneous administration offers convenience to patients since they can receive medications in a larger range of settings.
What was the design of the 3475A-D77study of subcutaneous pembrolizumab in NSCLC?
The multicenter, randomized, open-label trial that compared pembrolizumab through subcutaneous administration vs pembrolizumab through IV infusion enrolled patients who had a histologically or cytologically confirmed diagnosis of squamous or nonsquamous NSCLC and a life expectancy of at least 3 months.3 Patients were at least 18 years of age and were required to provide archival tumor tissue samples or newly obtained biopsies of tumor lesions that were not previously irritated.
If patients had a diagnosis of small cell lung cancer, received prior systemic anticancer therapy for metastatic NSCLC, received prior systemic anticancer therapy including investigational agents within 4 weeks before random assignment, or received prior radiotherapy within 2 weeks of start of study intervention, they were excluded from the study.
Patients in the subcutaneous arm of the trial received 790 mg of pembrolizumab formulated with berahyaluronidase alfa through subcutaneous administration in combination with platinum doublet chemotherapy on day 1 of each 6-week cycle for 18 cycles. Patients in the IV infusion arm of the trial received a 400-mg dose of pembrolizumab through IV infusion in combination with platinum doublet chemotherapy also on day 1 of each 6-week cycle for 18 cycles.2,3
The trial’s primary objectives were to measure the both the exposure and trough serum concentration of pembrolizumab in each arm to help determine whether subcutaneous administration of the drug was noninferior to IV pembrolizumab. Other secondary objectives of the trial were to evaluate the ORR, PFS, and OS between the 2 arms.
References
European Commission approves subcutaneous administration of Keytruda (pembrolizumab) for all adult indications approved in the European Union. News Release. Merck. November 19, 2025. Accessed November 20, 2025. https://www.merck.com/news/european-commission-approves-subcutaneous-administration-of-keytruda-pembrolizumab-for-all-adult-indications-approved-in-the-european-union/
Felip E, Rojas CI, Schenker M, et al. Subcutaneous versus intravenous pembrolizumab, in combination with chemotherapy, for treatment of metastatic non-small-cell lung cancer: the phase III 3475A-D77 trial. Ann Oncol. 2025;36(7):775-785. doi:10.1016/j.annonc.2025.03.012
A study of subcutaneous (SC) pembrolizumab coformulated with berahyaluronidase alfa (MK-3475A) vs intravenous pembrolizumab in adult participants with metastatic non-small cell lung cancer (NSCLC) (MK-3475A-D77). ClinincalTrials.gov. Updated September 11, 2025. Accessed November 20, 2025. https://clinicaltrials.gov/study/NCT05722015
Jay Woods, chief market strategist at Freedom Capital Markets, is eying a retailer which is both a holiday-shopping play and an earnings play this week: Dollar General . “It is now in a near-term uptrend with room to run,” said Woods ahead of the discount retailer’s earnings on Thursday. “Let’s see if they can get back above $115 — it’s got room to run if it does,” said the longtime trader. DG YTD mountain Dollar General, YTD If it pulls back on earnings, Woods said the $98 level is the one to watch to see if the “long-term turnaround story is intact.” Other things Woods is watching this week: Salesforce earnings on Wednesday after the bell: “It’s down 30% year to date, and technically at a key level. Watch $230. It’s tested three times now and held. We’re at that level as we go into the numbers. If we fall below that, it could be a rough start to 2026.” Results from MongoDB , Snowflake , CrowStrike , and Rubrik . S & P 500 is less then 2% from all-time highs A trickle of economic data before the Fed’s big decision next week. (See the video above for the full analysis from Woods.)
We are introducing new agentic capabilities in AWS Transform to accelerate organization-wide code and application modernization across any code, API, framework, runtime, architecture, language, and even company-specific programming languages and frameworks. With pre-built transformations for common patterns (e.g., Java, Node.js, and Python upgrades) and custom transformations for organization-specific tasks, a specialized agent executes consistent, repeatable, and high-quality transformations.
The FDA has granted priority review to a new drug application (NDA) seeking the approval of sonrotoclax (BGB-11417; BeOne Medicines) for the treatment of adult patients with relapsed or refractory mantle cell lymphoma (MCL) who have received prior treatment with a BTK inhibitor.1
The NDA is backed by findings from the phase 1/2 BGB-11417-201 trial (NCT05471843), which achieved its primary end point of overall response rate (ORR) per independent review committee (IRC) and showed clinically meaningful responses among 125 adult patients with relapsed/refractory MCL who had been previously treated with a BTK inhibitor. Positive outcomes were also seen across several secondary efficacy end points, such as complete response rate, duration of response (DOR), and progression-free survival (PFS). Regarding safety, the trial investigators deemed sonrotoclax to be well tolerated with manageable toxicity risks.
Data supporting the NDA and priority review designation will be presented at the 2025 ASH Annual Meeting.
Previously, in October 2025, the FDA granted sonrotoclax breakthrough therapy designation as a potential therapeutic option for the treatment of patients with relapsed or refractory MCL.2
“Sonrotoclax is advancing with remarkable speed, from breakthrough therapy designation to priority review, all within a short window,” Lai Wang, PhD, global head of Research & Development at BeOne Medicines, stated in a news release.1 “That pace reflects both the strength of the data and the urgency of the need for patients with relapsed/refractory MCL. With rapid, deep, and durable responses and a manageable safety profile, sonrotoclax is emerging as a potential best-in-class BCL-2 inhibitor, alongside our 2 other transformative hematology assets—BTK inhibitor Brukinsa [zanubrutinib] and investigational BTK degrader BGB-16673.”
What is the design of the BGB-11417-201 trial?
This global, multicenter, single-arm, open-label trial enrolled patients at least 18 years of age with histologically confirmed MCL who had received prior systemic treatment for MCL, including an anti-CD20 agent and a BTK inhibitor.3 Patients needed to have relapsed or refractory disease and the presence of measurable disease. They were also required to have available archival tissue that confirmed their MCL diagnosis or be willing to undergo fresh tumor biopsy. An ECOG performance status of 0 to 2 and adequate organ function were also required.
In part 1 of the trial, patients (n = 22) were treated with sonrotoclax at either 160 mg or 320 mg daily to evaluate the safety and tolerability of the agent and determine the recommended phase 2 dose (RP2D) for part 2.4 The primary end points in part 1 included the incidence of dose-limiting toxicities, treatment-emergent adverse effects (TEAEs), serious AEs, and tumor lysis syndrome.3 Secondary end points included pharmacokinetic outcomes.
Secondary end points investigated across both parts included investigator-assessed ORR; DOR, PFS, and time to response as assessed by investigators and the IRC; and overall survival.
Part 2 enrolled 103 patients, who received sonrotoclax at the RP2D of 320 mg daily following ramp-up dosing. The primary end point in part 2 was IRC-assessed ORR. Secondary end points specific to part 2 included the incidence of TEAEs and serious AEs; the number of patients with clinically significant changes from baseline in vital signs and clinical laboratory values; the number of patients with clinically significant physical examination findings; and quality of life measures.
What other regulatory next steps are planned for sonrotoclax?
BeOne Medicines plans to participate in the FDA’s Project Orbis for sonrotoclax. Project Orbis helps facilitate the concurrent submission and review of oncology products between international regulatory bodies.1 The company also plans to submit data from the BGB-11417-201 trial to other global regulatory agencies, including the European Medicines Agency, for the agent’s potential approval.
References
U.S. FDA grants priority review to sonrotoclax for the treatment of relapsed or refractory mantle cell lymphoma. News release. BeOne Medicines Ltd. November 26, 2025. Accessed November 26, 2025. https://ir.beonemedicines.com/news/us-fda-grants-priority-review-to-sonrotoclax-for-the-treatment-of-relapsed-or-refractory-mantle/786f1dad-0c9f-492e-9fce-f9ceadd24989
BeOne Medicines’ sonrotoclax granted breakthrough therapy designation by U.S. FDA. News release. BeOne Medicines. October 13, 2025. Accessed November 26, 2025. https://ir.beonemedicines.com/news/beone-medicines-sonrotoclax-granted-breakthrough-therapy-designation-by-us-fda/7a29ff75-4388-4f81-a23e-588149f94f9e
Study of BGB-11417 monotherapy in participants with relapsed or refractory mantle cell lymphoma. ClinicalTrials.gov. Updated September 9, 2025. Accessed November 26, 2025. https://clinicaltrials.gov/study/NCT05471843
BeOne Medicines announces positive topline results for sonrotoclax in relapsed or refractory mantle cell lymphoma (MCL). News release. BeOne Medicines. August 29, 2025. Accessed November 26, 2025. https://ir.beonemedicines.com/news/beone-medicines-announces-positive-topline-results-for-sonrotoclax-in-relapsed-or-refractory-mantle-cell-lymphoma/9b063914-3787-4b59-95fa-1e0941571f45