Qaasid News
Download Our App
Latest News from Pakistan
Oprah-Approved Brand Cozy Earth Added New Styles to Its Loungewear
February 4, 2026
2026 Preview: Arrow McLaren
February 4, 2026
Scientists find farthest galaxy ever detected – R&D World
February 4, 2026
Starmer orders release of files relating to Mandelson US ambassador decision | Peter Mandelson
February 4, 2026
Access Denied
February 4, 2026
Plan to release Mandelson documents approved after Labour MPs’ anger forces climbdown
February 4, 2026
MDT Boosts Survival Outcomes in Oligometastatic Prostate Cancer | Targeted Oncology
February 4, 2026
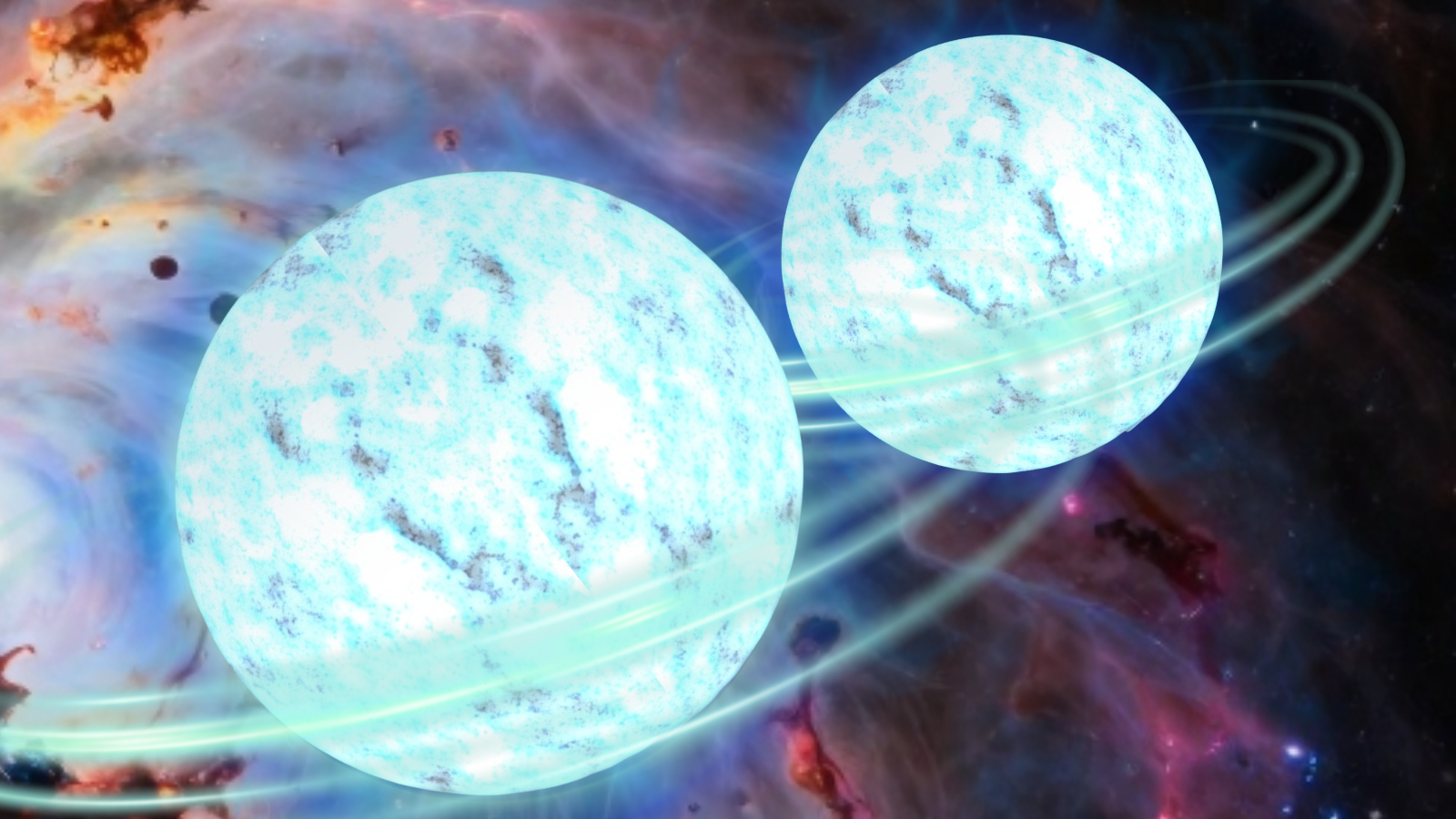
Watch dead neutron stars smash together in new NASA supercomputer simulation
February 4, 2026
Best smart scale deal: Save $50 on the Amzmerit smart scale at Amazon with code
February 4, 2026
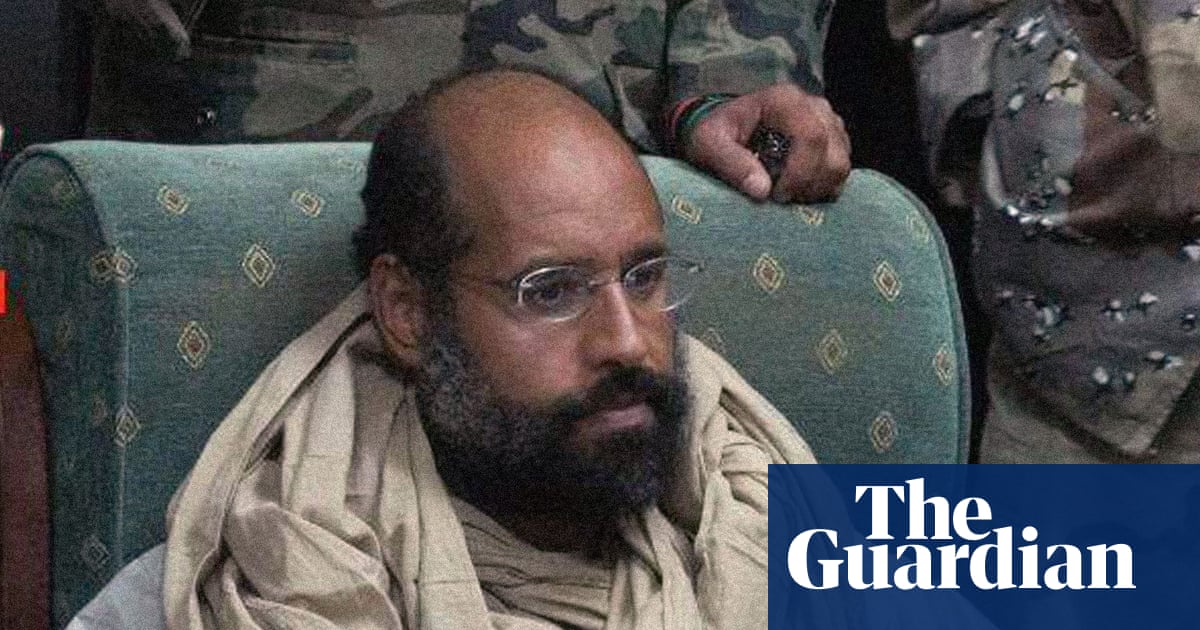
Murdered son of Muammar Gaddafi was perceived as a threat to Libya’s elite | Libya
February 4, 2026