Qaasid News
Download Our App
Latest News from Pakistan
CDF Munir says terrorists, facilitators will not be spared; no one can rationalise violence on any pretext – Dawn
February 4, 2026
Starmer to release sensitive Mandelson files after pressure – BBC
February 4, 2026
How Super Bowl halftime moments like the ‘wardrobe malfunction’ became flashpoints
February 4, 2026
Trump has attacked pillars of democracy, says Human Rights Watch – Reuters
February 4, 2026
Andrew Mountbatten-Windsor makes King Charles and Prince William implode
February 4, 2026
Become a GameChat pro with this guide – News – Nintendo Official Site
February 4, 2026
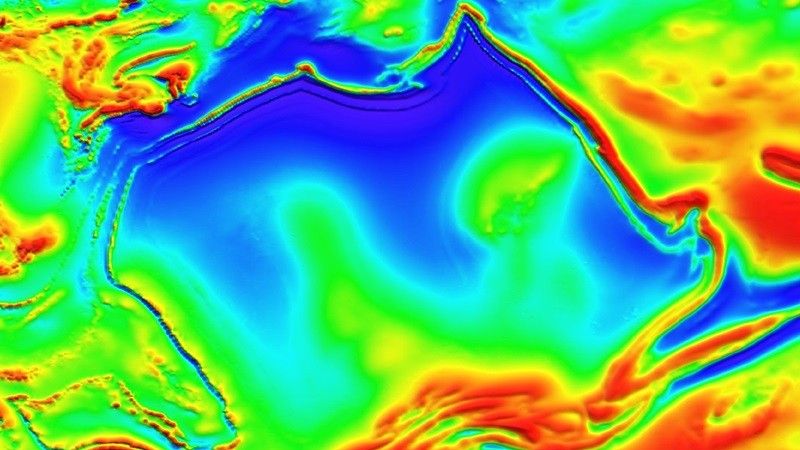
New map shows weird magnetic anomaly lurking beneath Australia’s Northern Territory
February 4, 2026
ASH 2025: Highlights in Relapsed/Refractory Multiple Myeloma
February 4, 2026
Rubio presses for broader Iran talks, voices doubt over deal
February 4, 2026
Best wearable deal: Save $100 on Samsung Galaxy Ring at Best Buy
February 4, 2026