Qaasid News
Download Our App
Latest News from Pakistan
Spin-heavy Pakistan hit form, but India boycott risks early T20 exit – France 24
February 4, 2026
Spin-heavy Pakistan Hit Form, But India Boycott Risks Early T20 Exit – Barron's
February 4, 2026
Honda Co-developing Automobile SoC with U.S.-based Mythic to Accelerate Research to Enhance AI Computing Performance and Energy Efficiency
February 4, 2026
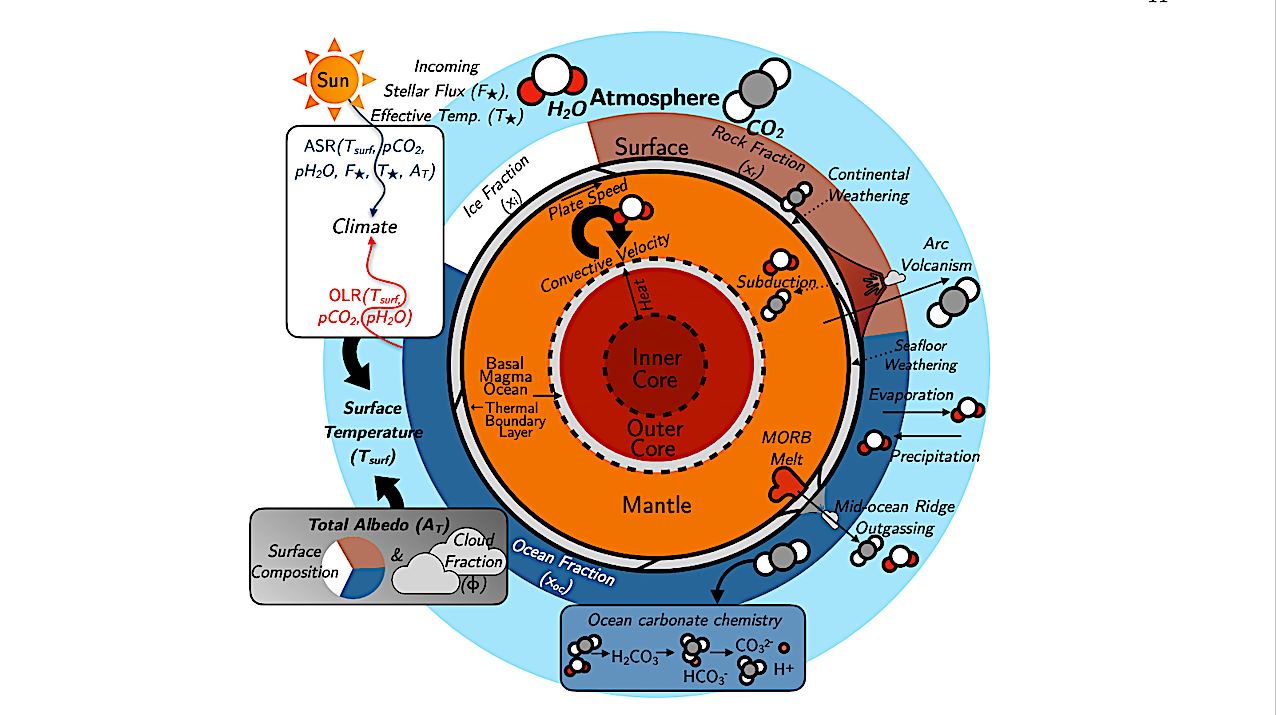
A Whole-planet Model Of The Earth Without Life For Terrestrial Exoplanet Studies
February 4, 2026
Group B Preview: Co-hosts’ big opportunity at T20 World Cup | ICC Men’s T20 World Cup, 2026
February 4, 2026
What the RBA wants Australians to do next to fight inflation – or risk more rate hikes
February 4, 2026
Soft-bodied fossil deposit in Hunan’s Huayuan fills gap in Earth’s history
February 4, 2026
Apple integrates Anthropic’s Claude and OpenAI’s Codex into Xcode 26.3 in push for ‘agentic coding’ – Venturebeat
February 4, 2026
Elon Musk calls Spanish PM a ‘tyrant’ over plan to ban under-16s from social media and curb hateful content | Social media
February 4, 2026
Dyson’s Thinnest and Lightest Cordless Vacuum Ever Is Finally Ready to Buy in the US
February 4, 2026