Qaasid News
Download Our App
Latest News from Pakistan
Texas Tech posts another record semester in classroom
January 7, 2026
Shortlist announced for Biblio-Buzz 2026 – The Alexandra Palace Children’s Book Award
January 7, 2026
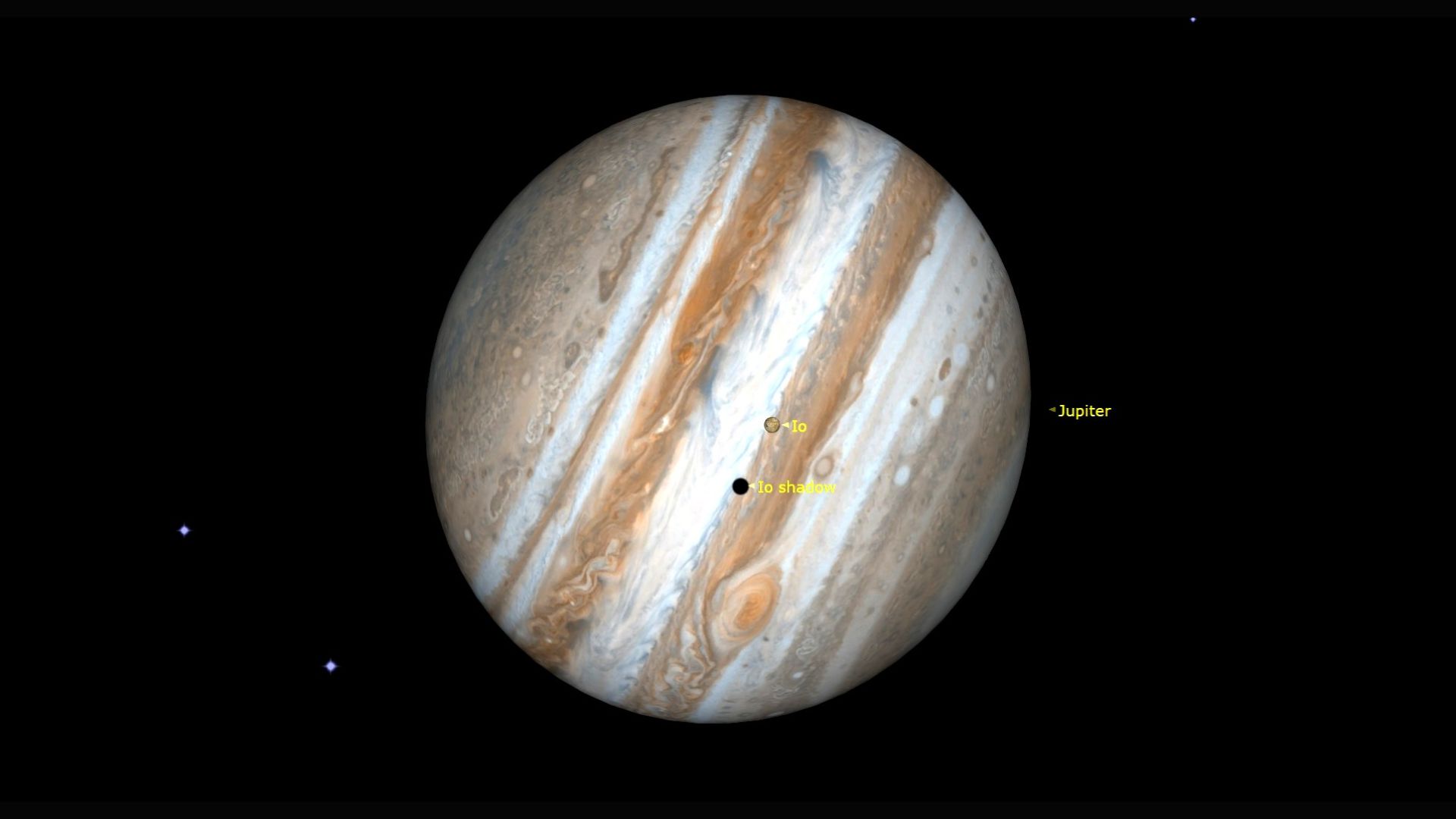
January belongs to Jupiter: See the king of planets in the night sky this month
January 7, 2026
Sobi to advance Gamifant® (emapalumab) in interferon-gamma-driven sepsis (IDS) based on EMBRACE topline data
January 7, 2026
PM Shehbaz Sharif to visit Quetta, inaugurate Danish School and review security
January 7, 2026
Your everyday food may be rewriting your liver’s future and scientists say the risk builds quietly over time
January 7, 2026
Reflagged by Russia, spied on by UK, seized by US: why so much interest in a rusty tanker in the Atlantic? | Water transport
January 7, 2026
Rubio says he will meet with Denmark about Greenland next week
January 7, 2026
New study examines a gravitational wave mystery | CU Boulder Today
January 7, 2026
Fossils found in Moroccan cave may be a close Homo sapiens ancestor – Reuters
January 7, 2026