Qaasid News
Download Our App
Latest News from Pakistan
A Doctor’s Guide to Longevity Supplements and Aging Well
February 2, 2026
Google’s Latest AI Search Features Look Like a Personalized Travel Concierge
February 2, 2026
In major Punjab police shake-up, Rao Abdul Kareem appointed new IG
February 2, 2026
Emma Raducanu: Briton records first win since Australian Open and coach split
February 2, 2026
ADDICT-ICCU: Recreational Drug Use Predicts MACE Risk Post ICCU
February 2, 2026
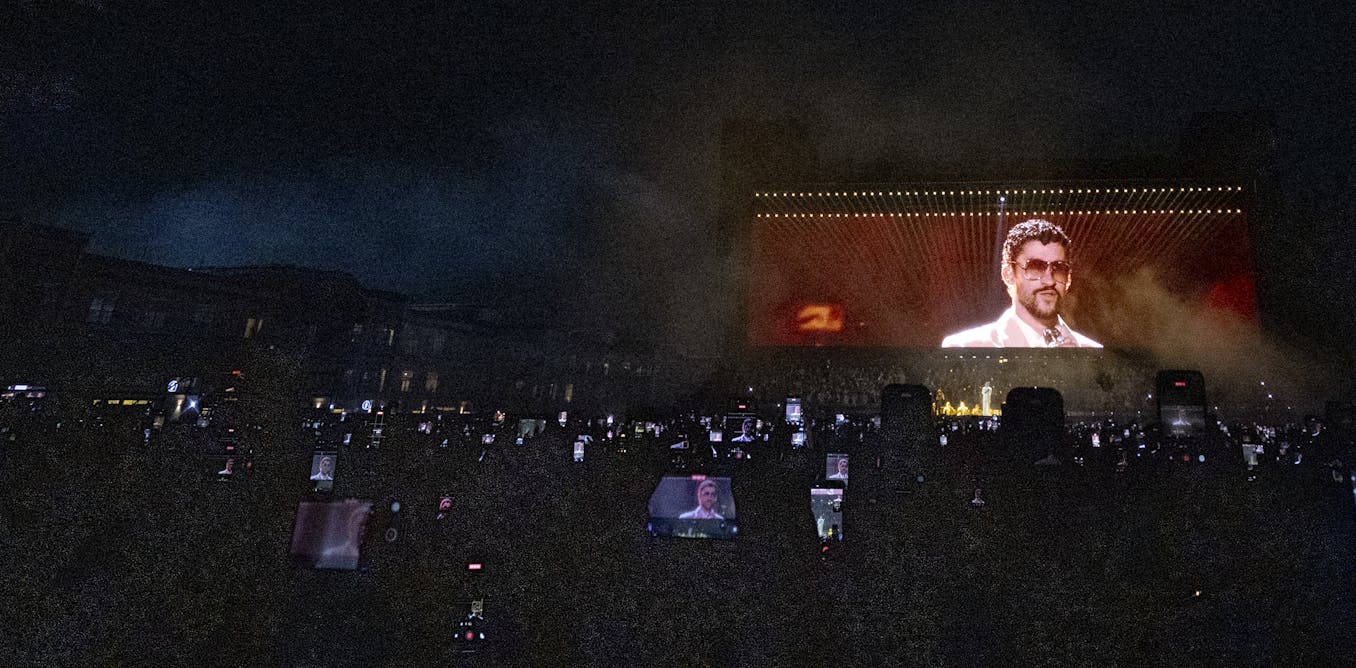
Bad Bunny’s Super Bowl show is part of long play drawn up by NFL to score with Latin America
February 2, 2026
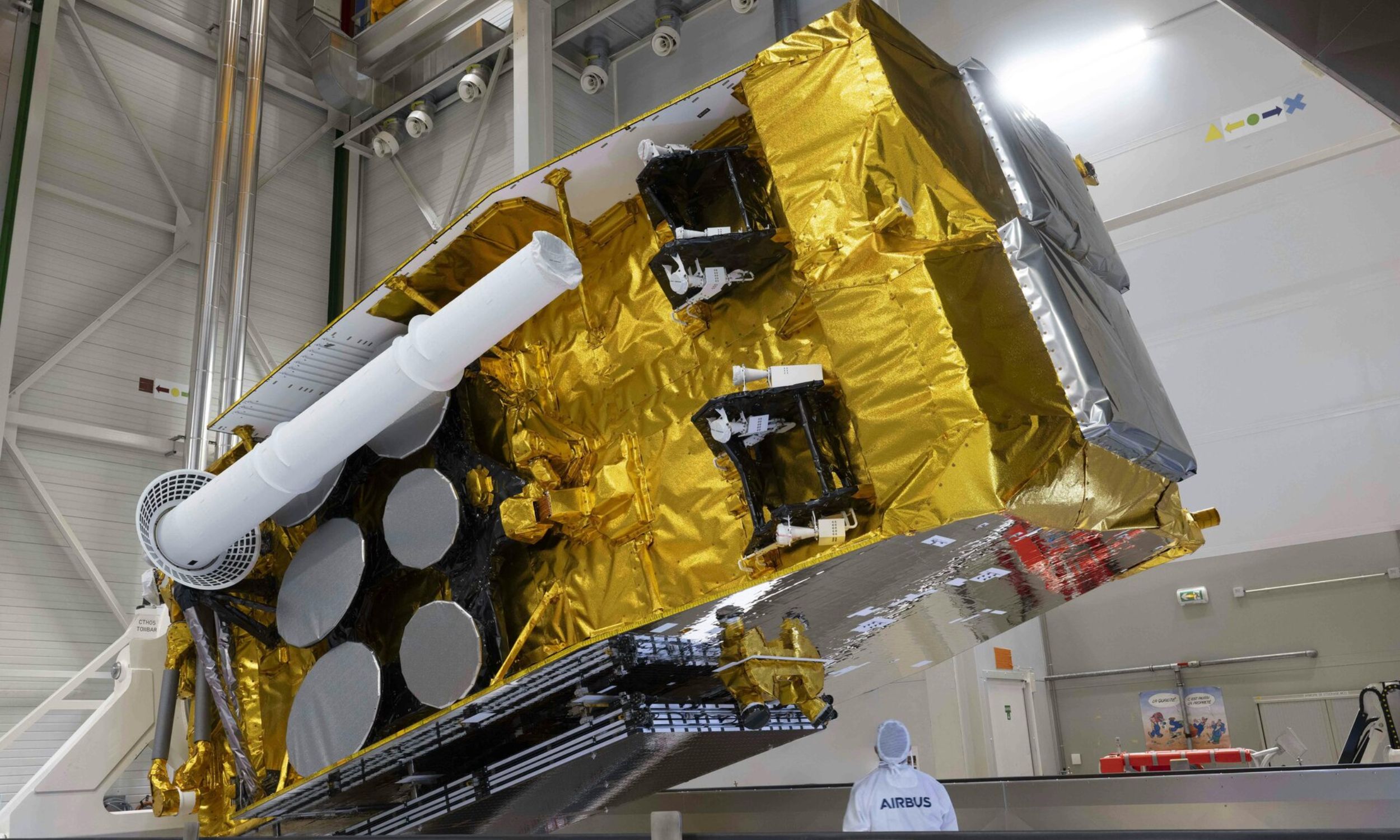
Tiny particle damages military satellite worth millions
February 2, 2026
Gaza: Limited Rafah crossing reopening sparks hope – but also ‘massive trepidation’ – UN News
February 2, 2026
Margot Robbie’s Chanel Wuthering Heights Dress Was Inspired by the Red Carpet Itself
February 2, 2026
How vines search for and attach to other plants
February 2, 2026