Qaasid News
Download Our App
Latest News from Pakistan
Ifunanya Nwangene: Aspiring Nigerian singer dies after snakebite in Abuja – BBC
February 1, 2026
Grammys 2026 winners: The complete list
February 1, 2026
Luke Littler ‘greatest darts player ever’ says Luke Humphries after teenager’s World Masters win
February 1, 2026
Pricing, Storage & Features Compared
February 1, 2026
Can AI discover new art forms through mathematical rules?
February 1, 2026
Philips intros ENVIA 27M25500XD: claims the world's first 1000Hz gaming monitor spot – TweakTown
February 1, 2026
‘Made me want to punch the air’: The Night Manager’s seductive, twisty return was a TV triumph | The Night Manager
February 1, 2026
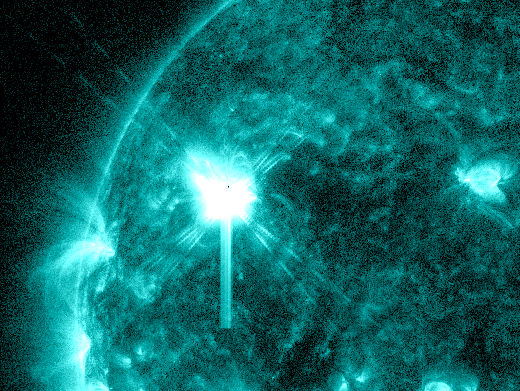
Major Solar Flare Strikes as Giant New Sunspot Erupts
February 1, 2026
Artificial organ keeps patient alive for 48 hours after removal of bilateral lungs-Xinhua
February 1, 2026
Statement Following Decision to Reduce HGV Tournament of Champions to 54 Holes – LPGA
February 1, 2026