Qaasid News
Download Our App
Latest News from Pakistan
Pakistan committed to conservation, sustainable management of wetlands: President – RADIO PAKISTAN
February 2, 2026
Winners and nominees at the 2026 Grammy Awards – updating live – BBC
February 2, 2026
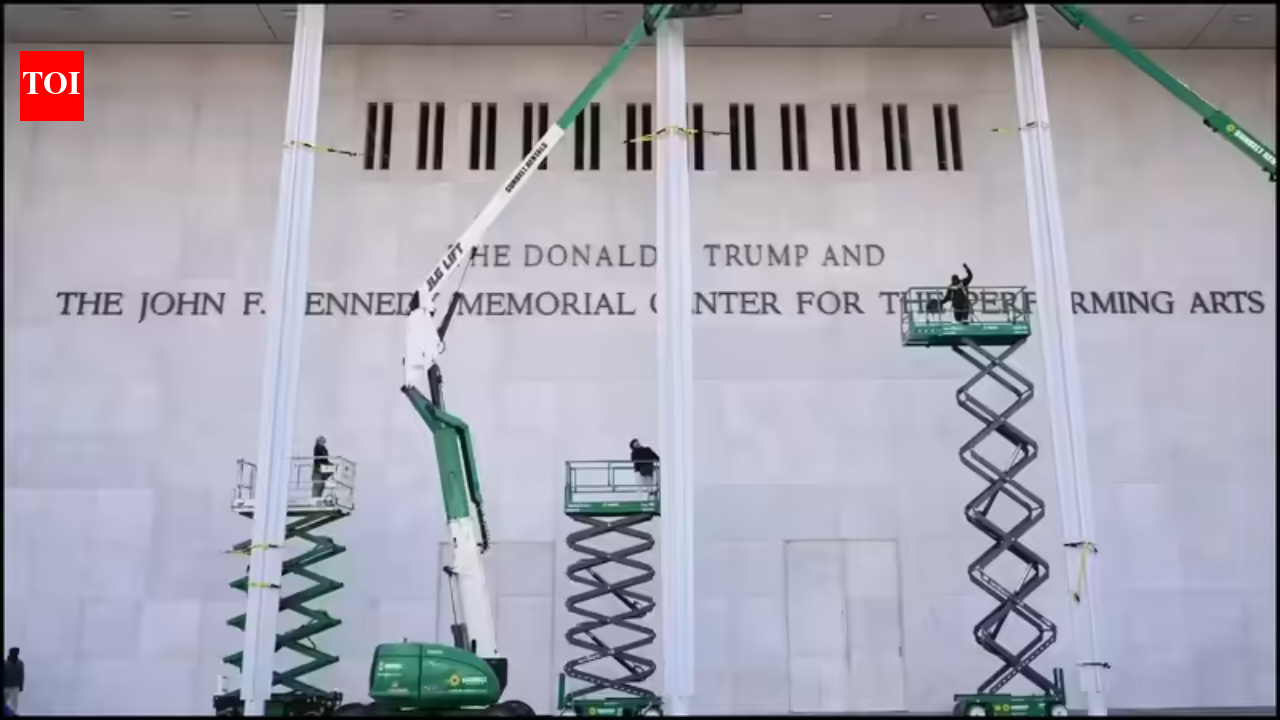
‘Tired, broken, and dilapidated’: Donald Trump announces two-year shutdown of Kennedy Center for ‘complete rebuilding’
February 2, 2026
SCIRP Open Access
February 2, 2026
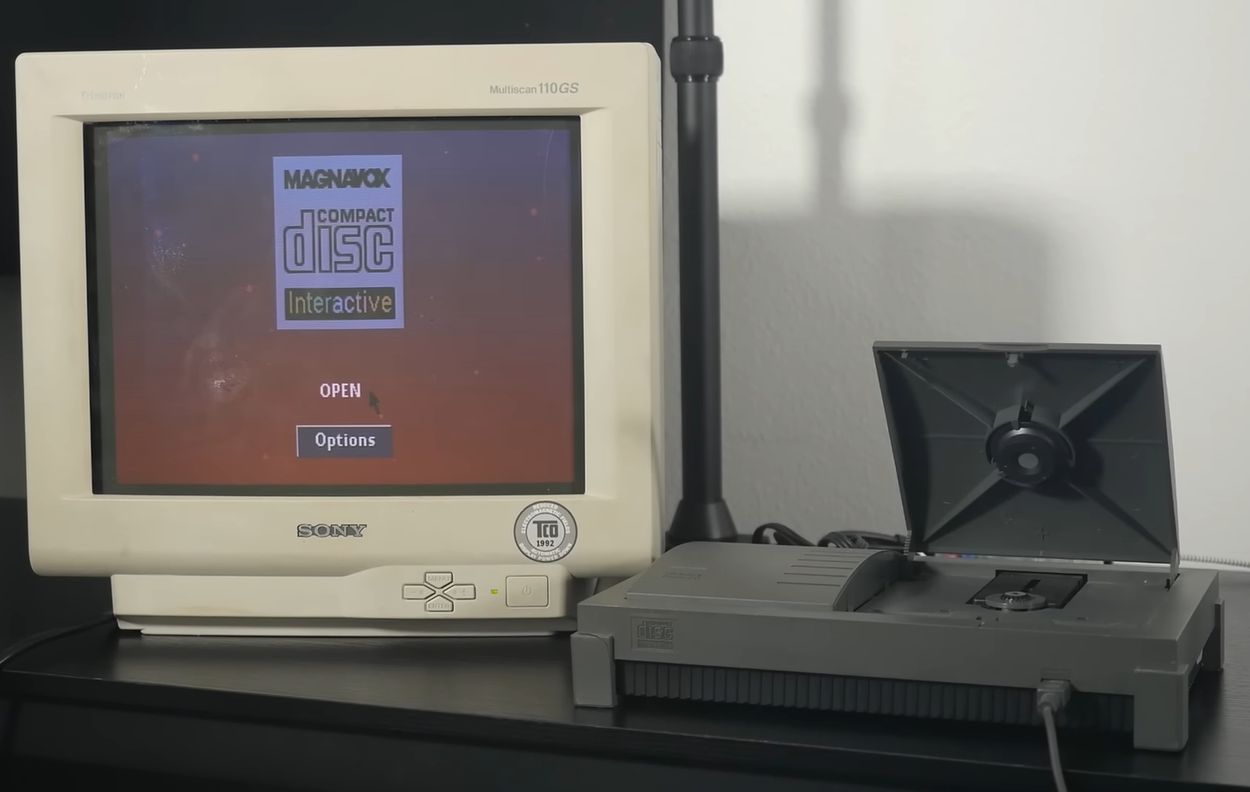
Fixing Sony And Philips’ Doomed CD-i Console
February 2, 2026
U.S. first lady documentary “Melania” receives mixed views on opening-Xinhua
February 2, 2026
Basant festival: rooftop rentals surge in Walled City – Business Recorder
February 2, 2026
Justin Bieber performs nearly naked in boxers at 2026 Grammys
February 2, 2026
SCIRP Open Access
February 2, 2026
Which smartphone was the world’s best-seller in 2025?
February 2, 2026