Qaasid News
Download Our App
Latest News from Pakistan
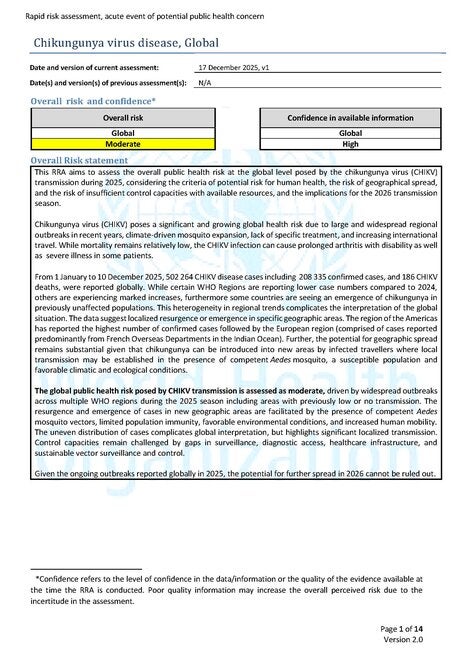
WHO Rapid Risk Assessment – Chikungunya virus disease, Global v.1 – PAHO/WHO
December 29, 2025
Got a gift card this holiday? Here’s how to trade it in or redeem it for cash.
December 29, 2025
New computational method “Fast-Tracks” drug discovery
December 29, 2025
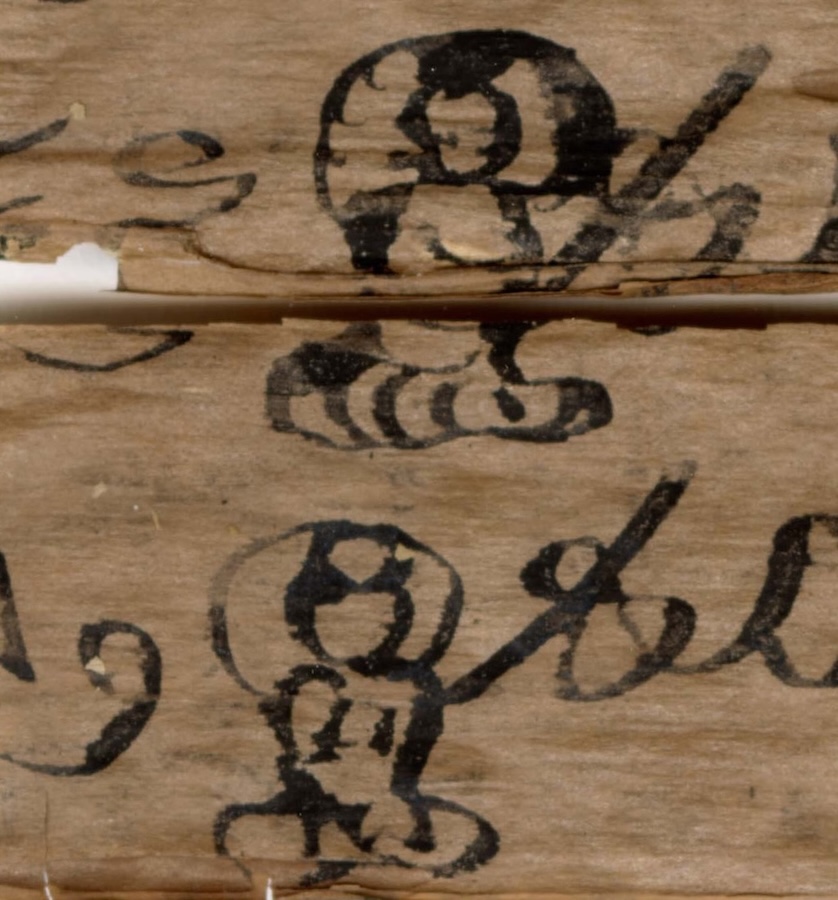
Buddhist Heritage: Khyentse Foundation to Extend Support for Conservation of Gandhari Scrolls at Islamabad Museum
December 29, 2025
The Year in Image Generation
December 29, 2025
Let 2026 be the year the world comes together for AI safety
December 29, 2025
Comparative Evaluation of mNGS and Traditional Culture Methods in Path
December 29, 2025
What Creative Custom Pool Float Shapes Are Trending in 2026?
December 29, 2025
The unhealthy reproductive system of infertile women after IVF-ET caus
December 29, 2025
Access Denied
December 29, 2025