Qaasid News
Download Our App
Latest News from Pakistan
New nonstop flights from Austin coming in 2026
December 29, 2025
Andy Zaltzman: ‘Aristophanes is total comedy: political satire, slapstick and dick jokes’ | Stage
December 29, 2025
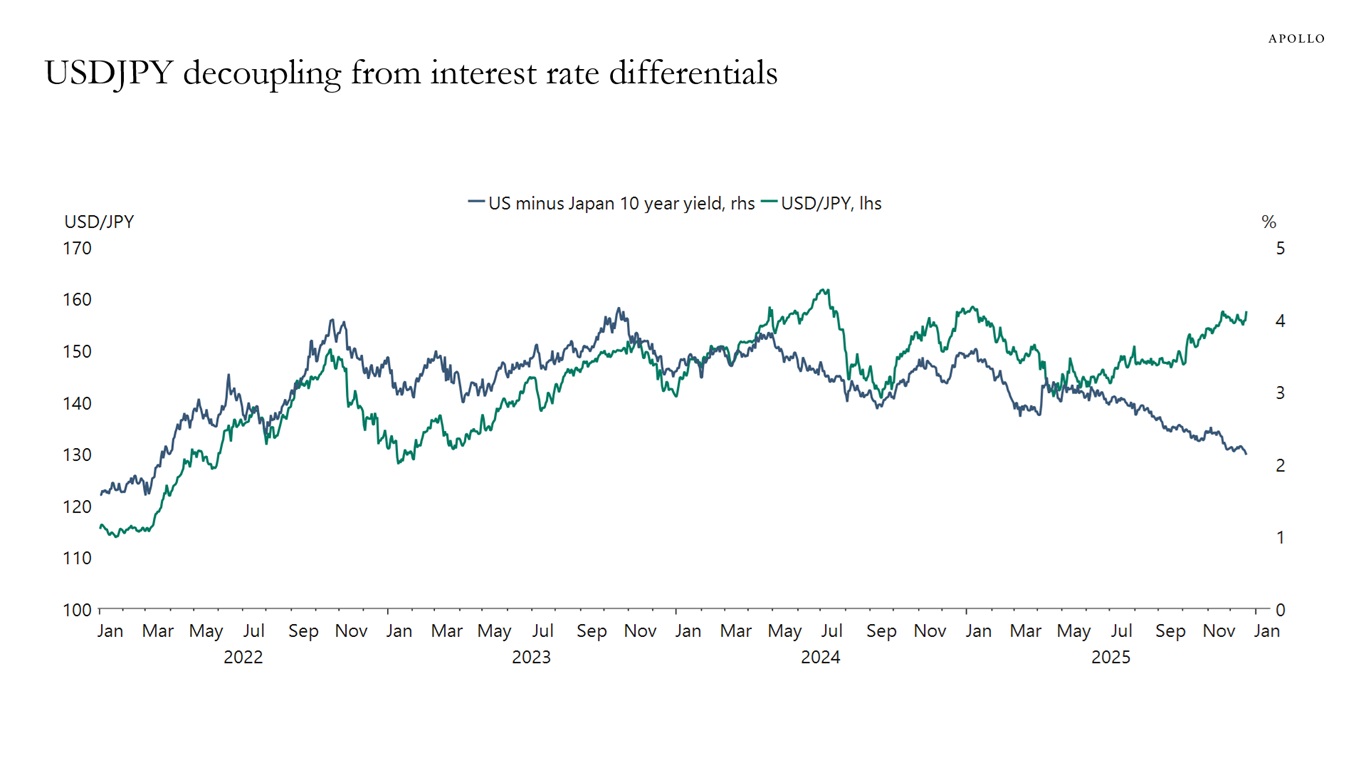
Yen Much Weaker Than Interest Rate Differentials Would Have Predicted
December 29, 2025
Hidden causes of depression you may not know
December 29, 2025
Statement by HRVP Kallas and Commissioner Kos on Kosovo parliamentary elections – European Commission
December 29, 2025
Hormone therapy has “no impact” on dementia risk, study finds
December 29, 2025
Wild things we learned about Earth in 2025
December 29, 2025
South Asia’s Dairy Intolerance Could Help Explain Our Ability to Drink Milk : ScienceAlert
December 29, 2025
Podcast tours are all the rage: Inside the big business of live shows
December 29, 2025
Even ‘Avatar: Fire and Ash’ can’t lift 2025 box office out of pandemic-crisis doldrums
December 29, 2025