Qaasid News
Download Our App
Latest News from Pakistan
This Week on NeurologyLive® — December 29, 2025 | NeurologyLive
December 29, 2025
How AI Could Help Your Grocery Shopping Experience With Nutrition Information
December 29, 2025
Cristiano Ronaldo reveals bold career target after Best Middle Eastern Player win
December 29, 2025
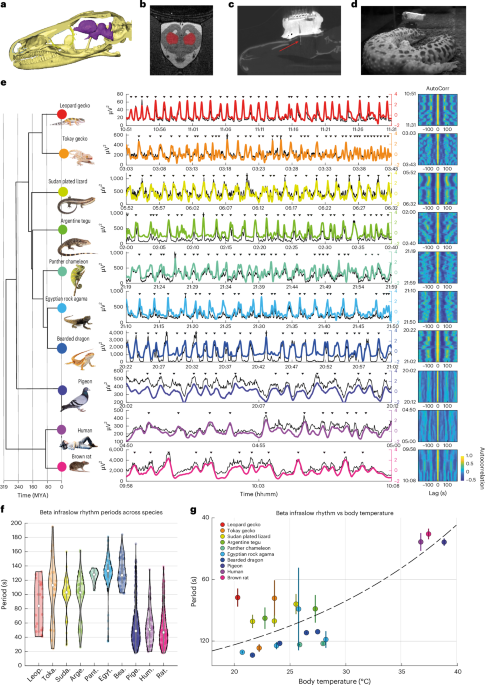
Sleep-dependent infraslow rhythms are evolutionarily conserved across reptiles and mammals
December 29, 2025
Giant ‘spider’ right in the middle of Europa’s Manannán crater proof of water? Scientists say…
December 29, 2025
2 Minute Medicine Rewind December 29th, 2025 – 2 Minute Medicine
December 29, 2025
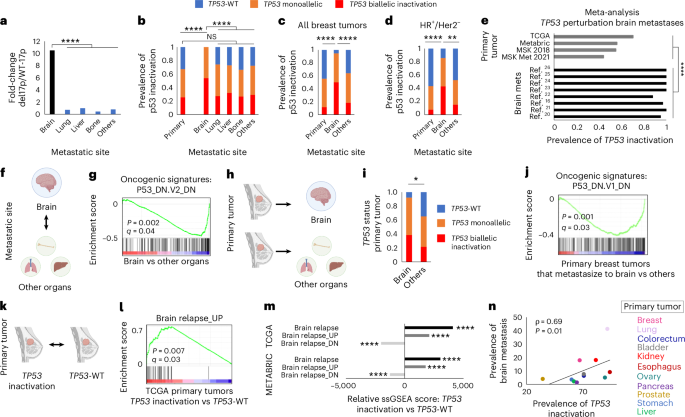
p53 inactivation drives breast cancer metastasis to the brain through SCD1 upregulation and increased fatty acid metabolism
December 29, 2025
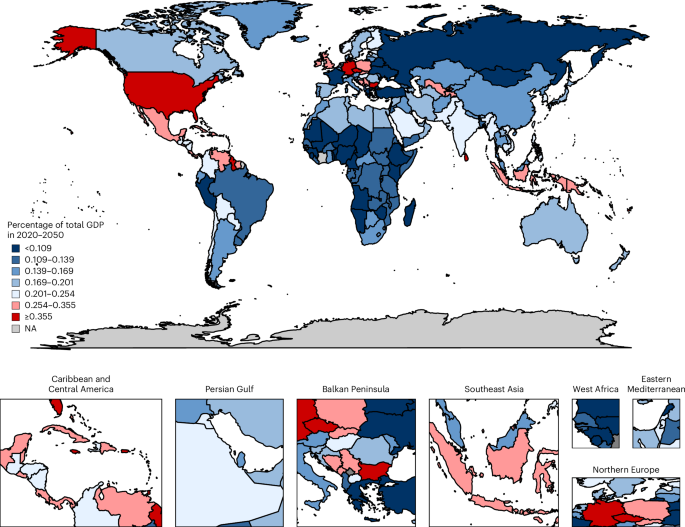
The global macroeconomic burden of diabetes mellitus
December 29, 2025
Osborne Clarke advises ALER Milano in the €200 million+ mixed concession for energy redevelopment and EPC services for a substantial public housing portfolio
December 29, 2025
New nonstop flights from Austin coming in 2026
December 29, 2025