Qaasid News
Download Our App
Latest News from Pakistan
Bad Bunny Turns Into a Schiaparelli Boy at the 2026 Grammys
February 2, 2026
PACED’s Summary Digest for Palliative Care Professionals – January 2026
February 2, 2026
A Tearful Shaboozey Shouts Out His Parents, Ancestors Backstage At The Grammys – Forbes
February 2, 2026
Indian banks prep for new provisioning norms with strong asset quality, capital – S&P Global
February 2, 2026
Edifier Launches MR5 Studio Speakers: Pro-Grade Audio Arrives in Australia
February 2, 2026
World Wetlands Day: Ministry vows wetlands’ restoration to reduce flood risks – Business Recorder
February 2, 2026
Grammys 2026 Live Updates and Red Carpet: Kendrick Lamar and Leon Thomas Win Early Awards – The New York Times
February 2, 2026
Addison Rae Channels Marilyn Monroe in White Alaïa at the Grammys
February 2, 2026
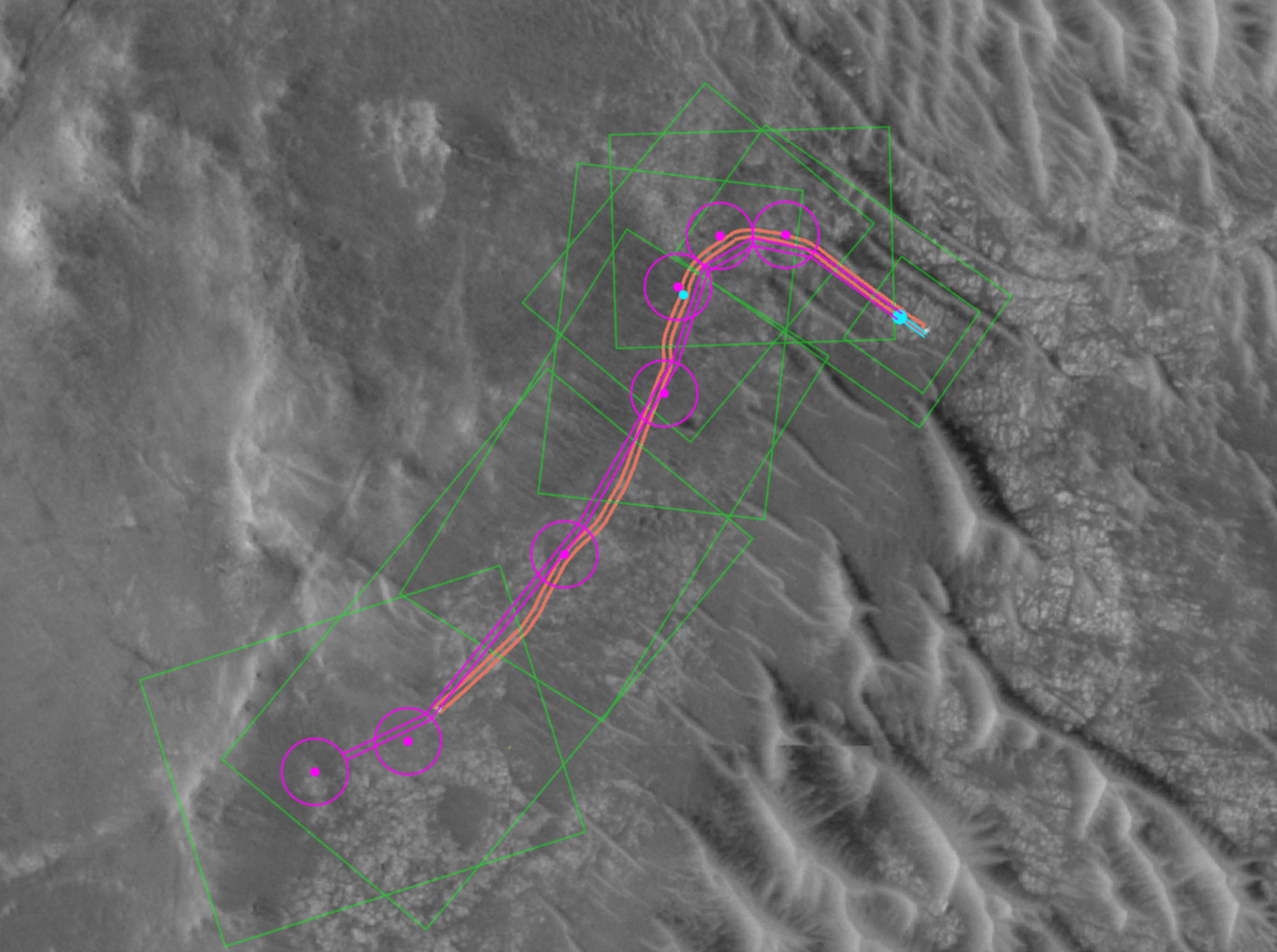
NASA uses Claude to plan first AI rover drives on Mars
February 2, 2026
NVIDIA releases important GeForce Security Update Driver for GeForce GTX 10 Series GPUs – TweakTown
February 2, 2026