Qaasid News
Download Our App
Latest News from Pakistan
Access Denied
February 7, 2026
Six great reads: romance fraud, pie and mash, and a road sign design genius |
February 7, 2026
Pakistan bowls first against Netherlands in T20 World Cup opener – The Washington Post
February 7, 2026
TV tonight: the return of a sparkling Scottish comedy | Television & radio
February 7, 2026
Live: Trump hails ‘very good’ Iran talks, says negotiations will continue early next week – France 24
February 7, 2026
Apple’s redesigned MacBook Pro can’t come soon enough
February 7, 2026
From Lord of the Flies to Deftones: your complete entertainment guide to the week ahead | Culture
February 7, 2026
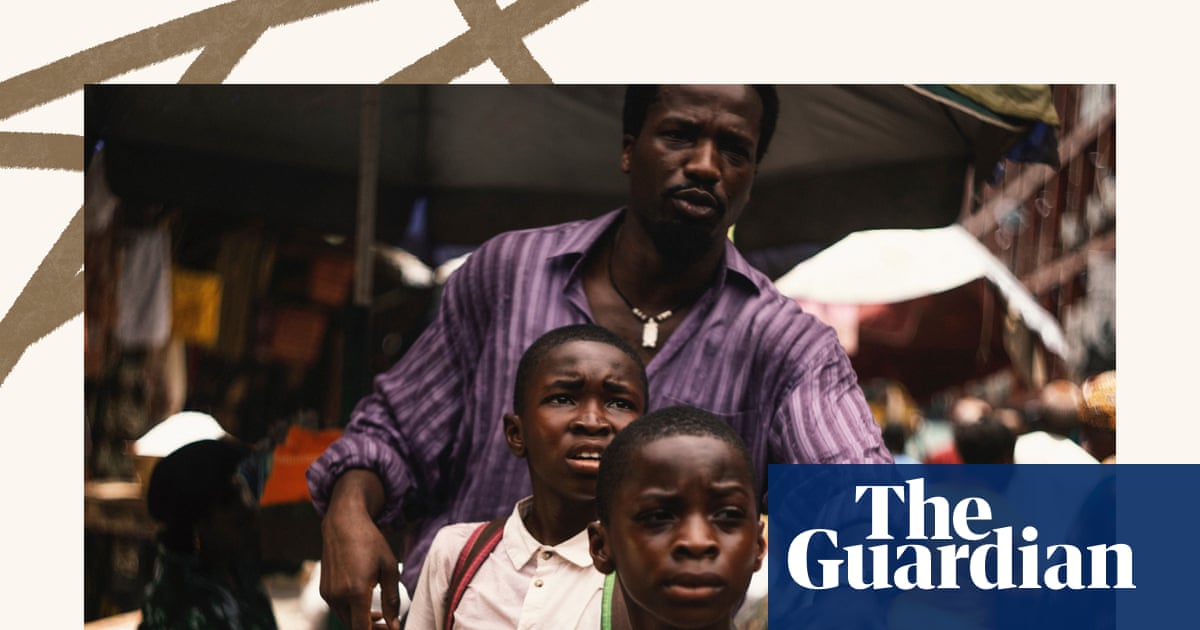
My Father’s Shadow to Hamlet: the week in rave reviews | Culture
February 7, 2026
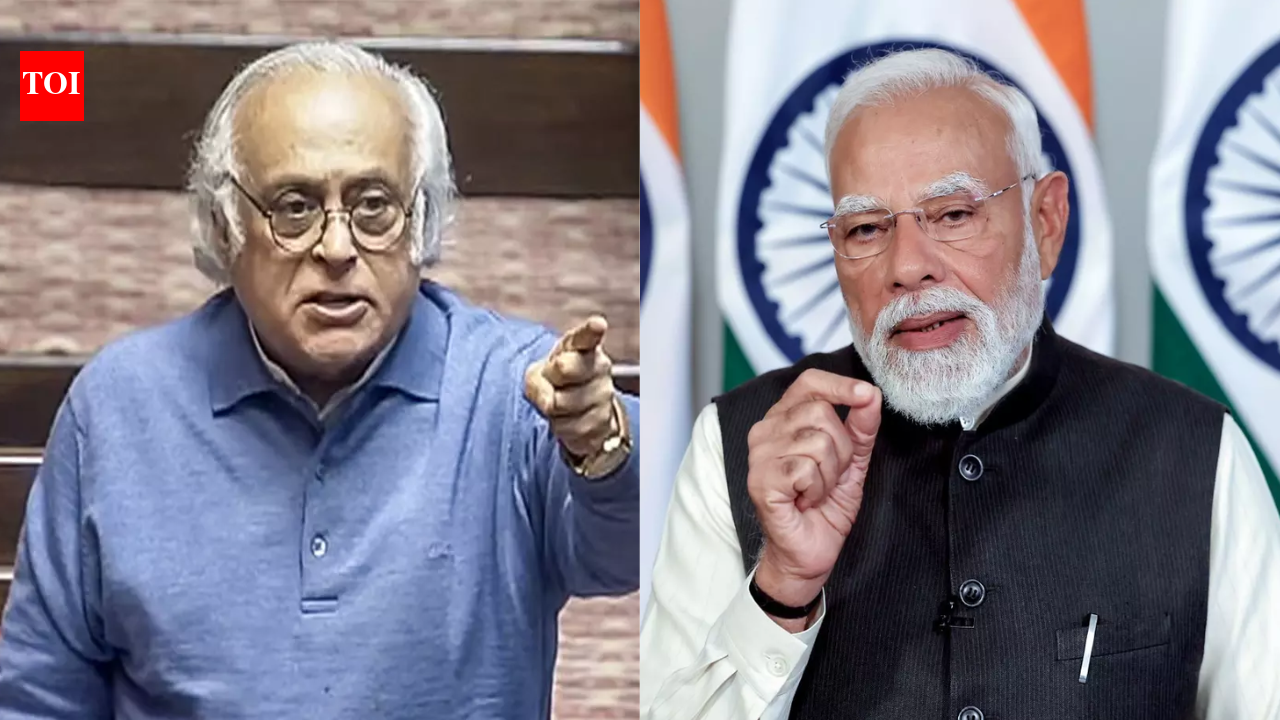
‘Dost dost na raha’: Congress takes filmy jibe at India-US trade deal; poses 5 questions | India News
February 7, 2026
Vietnam Airlines, Emirates, and Singapore Airlines Are Flocking to Hanoi for the Happy Tet 2026 – What the World’s Top Airlines See in This Historic Event!
February 7, 2026