Qaasid News
Download Our App
Latest News from Pakistan
Punjab govt to provide free public transport during Basant festival
January 31, 2026
Elon Musk's SpaceX applies to launch 1m satellites into orbit – BBC
January 31, 2026
Ipswich Town vs Preston North End: Championship stats & head-to-head
January 31, 2026
King Charles personally raises charity money, looks away from deeper problems
January 31, 2026
1152 zones for under $350?
January 31, 2026
Access Denied
January 31, 2026
What You Need To Know About Nipah Virus, Which Is Currently Surging In South Asia – Forbes
January 31, 2026
Access Denied
January 31, 2026
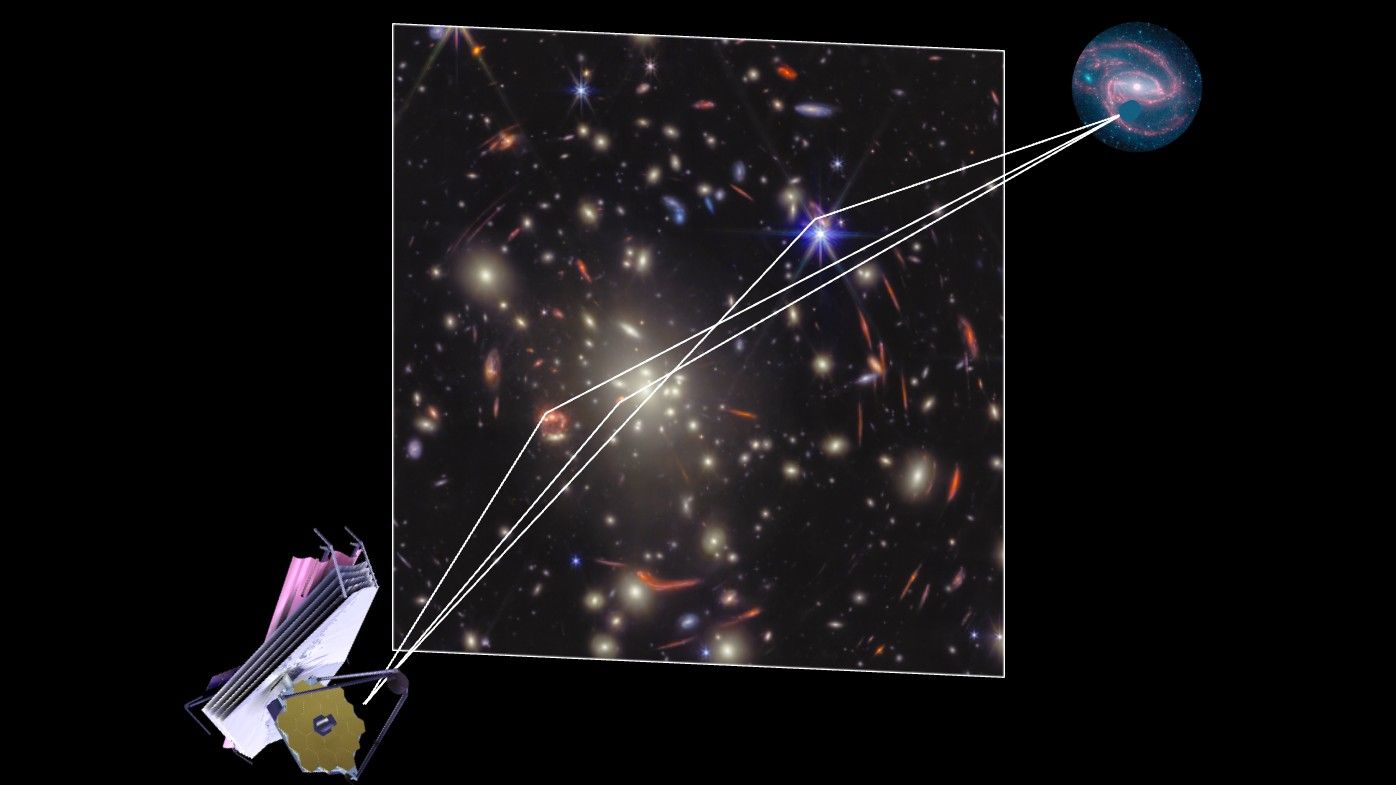
Supernova whose light will ‘reappear’ in 60 years could solve the biggest problem in cosmology
January 31, 2026
A Near-Mint Microsoft Surface Laptop 3 With Touchscreen Display Is Just $400 – PCMag
January 31, 2026