Qaasid News
Download Our App
Latest News from Pakistan
Six more children die in Tharparkar, monthly toll reaches 50
January 31, 2026
Christina Koch’s long road to the moon, from Antarctic ice to NASA’s Artemis 2
January 31, 2026
Chinese astronomers unveil birthplace environment of mysterious cosmic burst-Xinhua
January 31, 2026
New nasal spray vaccine efficiently prevents influenza
January 31, 2026
Former US Army Colonel Douglas Macgregor calls ‘Board of Peace’ a graft, claims Pakistan paid to join
January 31, 2026
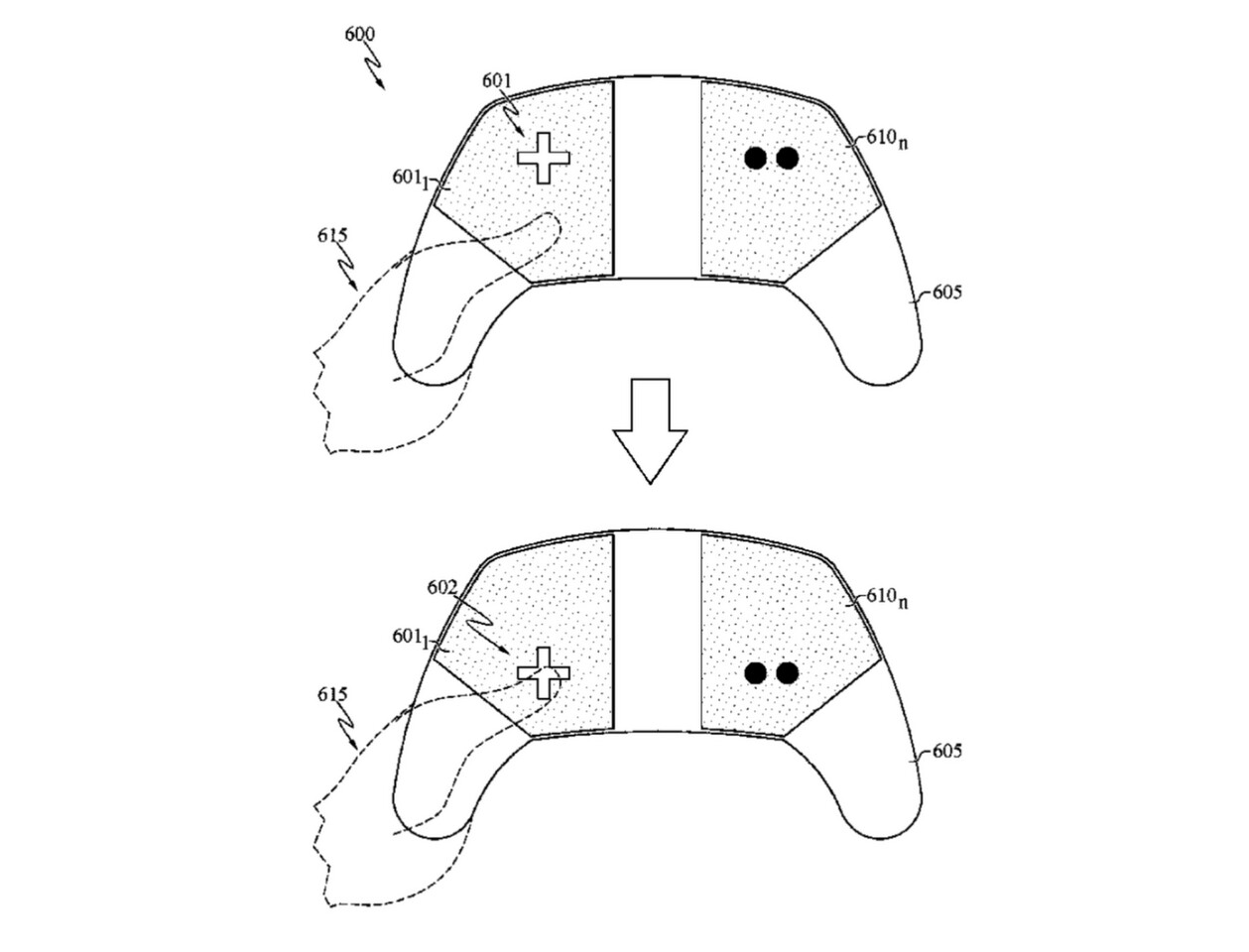
Sony Patents Buttonless Adaptive Controller With Customizable Layouts
January 31, 2026
United States approves major arms deals to Saudi Arabia, Israel – Dawn
January 31, 2026
TV tonight: Phil Collins reveals his health issues and 24-hour live-in nurse | Television & radio
January 31, 2026
Reinforcement Learning’s Scaling Problem, From Atari To The Real World
January 31, 2026
One KP father’s story challenges polio myths
January 31, 2026