Qaasid News
Download Our App
Latest News from Pakistan
Anthems, agency and arias: baritone Davóne Tines on rewriting his role – and the rules | Classical music
February 7, 2026
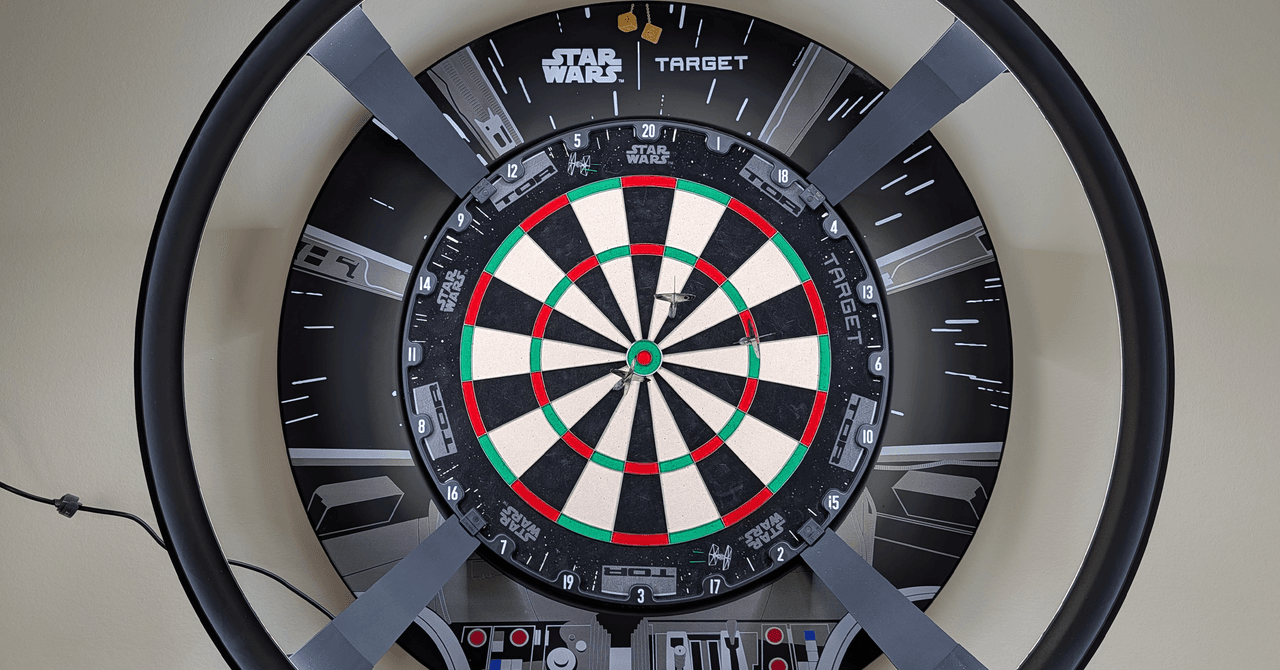
Target Darts Omni Auto Scoring System Hits the Mark
February 7, 2026
February 7, 2026 – Ciampa Defends TNT Title in 3-Way, 8-Man Parking Lot Fight, More
February 7, 2026
Syria, Saudi Arabia sign strategic deals, launch joint airline to boost investment, connectivity-Xinhua
February 7, 2026
Minibus crash kills 12 in northeastern Afghanistan – Arab News
February 7, 2026
Araghchi: Iran will strike US bases in Mideast if attacked
February 7, 2026
TikTok’s favourite headphones are 20% off
February 7, 2026
SC fixes 13 petitions involving Imran, Bushra Bibi for Monday hearing
February 7, 2026
Saturday Citations: Imaginative bonobos; cannabis brain benefits; sneaky beetles – Phys.org
February 7, 2026
Five stocks with more upside based on their latest earnings
February 7, 2026