Qaasid News
Download Our App
Latest News from Pakistan
Black fungus living at Chernobyl has evolved to “eat” radiation
December 21, 2025
Royal Variety Peformance an ‘unexpected surprise’ for NI singers
December 21, 2025
Taskmaster Champion of Champions 4 – press pack interviews
December 21, 2025
Francis’ Game-Winnings Three Lifts Rutgers Past Penn, 70–69
December 21, 2025
Peace Dialogue in Delhi Flags Deepening Kashmir Alienation, Urges Centre to Honour Statehood Promise
December 21, 2025
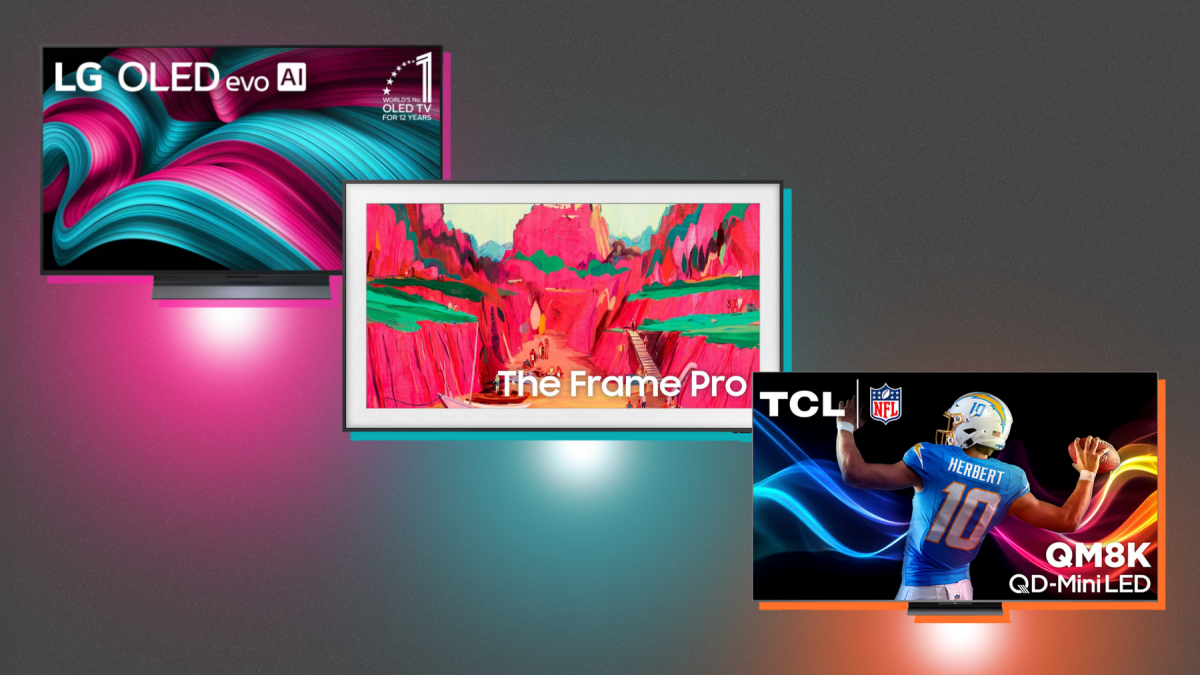
Best 65-inch+ TVs 2025: What to buy on Black Friday for watching sports, movies, more
December 21, 2025
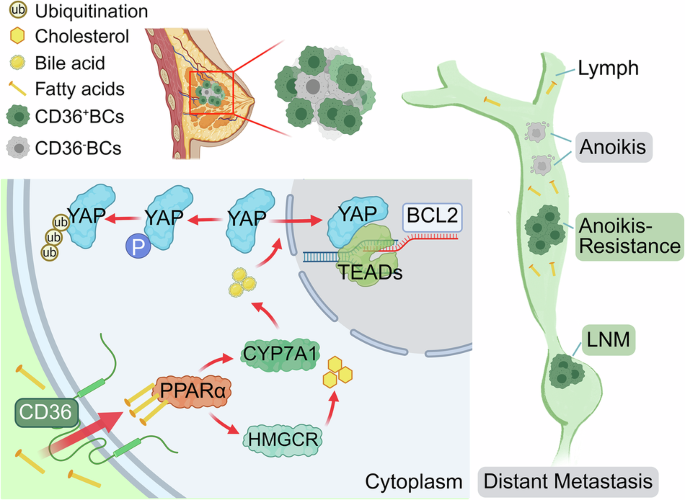
Elevated CD36 drives lymph node metastasis of breast cancer by activating Hippo-YAP signaling-mediated anoikis resistance
December 21, 2025
Apple’s Upgrade Decision—Hundreds Of Millions Of iPhones Affected – Forbes
December 21, 2025
‘Afghanistan will have to choose either Fitna al-Khawarij or Pakistan’ – RADIO PAKISTAN
December 21, 2025
Lee Cataluna: How A Small Incident On Kauaʻi Made Headlines Everywhere
December 21, 2025