Qaasid News
Download Our App
Latest News from Pakistan
How the World of Work Will Change Over the Next 20 Years – The Wall Street Journal
December 20, 2025
Galaxy Z Flip 8 tipped to be Samsung’s best flip phone with THIS Exynos chip
December 20, 2025
Carmen Monge-Montero: What NOT to Say to Someone With Cancer and What to Say Instead
December 20, 2025
Netanyahu plans to brief Trump on possible new Iran strikes, NBC News reports – Reuters
December 20, 2025
Prince William ‘honoured to become SAS charity patron’
December 20, 2025
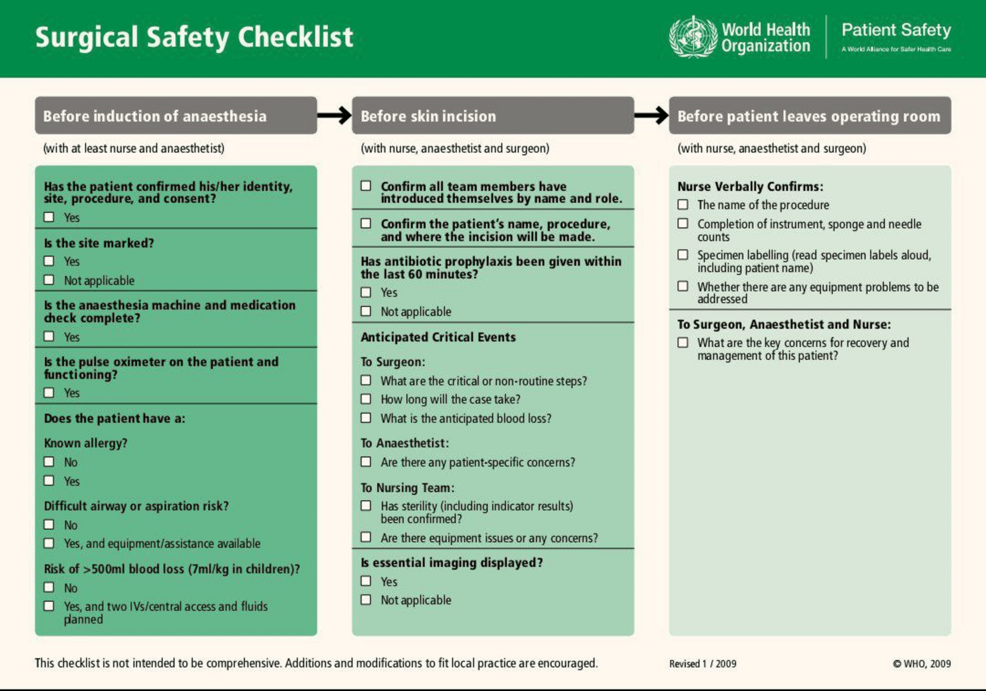
Improving Surgical Safety Through Checklist Compliance: Lessons From a Clinical Audit in a Teaching Hospital
December 20, 2025
How kangaroos hop faster without using more energy
December 20, 2025
Renormalization Group Flow Irreversibility Enables Constraints On Effective Spatial Dimensionality
December 20, 2025
Men’s brains may age faster than women’s, suggests major new study
December 20, 2025
At least 8 dead and dozens wounded in Russian strike on Ukraine’s Odesa port
December 20, 2025