Qaasid News
Download Our App
Latest News from Pakistan
Tomodachi Life: Living the Dream Direct spotlights quirky fun with player-made Mii characters
January 30, 2026
AI helps doctors spot breast cancer in scans
January 30, 2026
Maternal Stroke Recovery Shows Mixed Long-Term Outcomes – Medscape
January 30, 2026
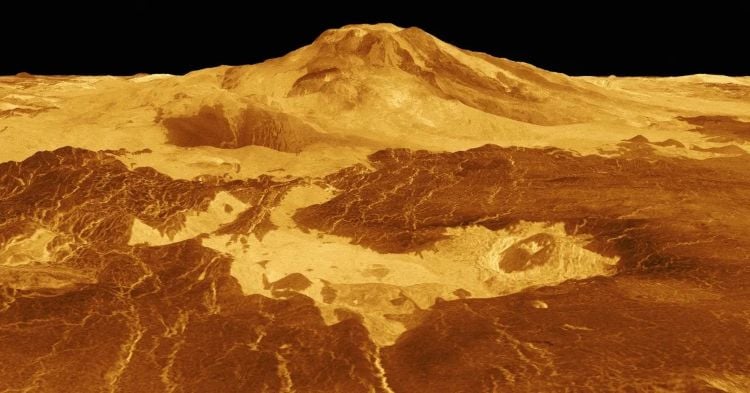
Venus Might Harbor Massive Subsurface Lava Tunnels
January 30, 2026
Asia’s mountains were born before Dinosaurs knew it: The lost Tethys ocean behind today’s landscape
January 30, 2026
Trump says ‘very dangerous’ for UK to do business with China, after Starmer hails progress in Beijing | China
January 30, 2026
Astronomers spot new Earth-sized planet near habitable zone 146 light-year away
January 30, 2026
India ordered to submit hydropower records sought by Pakistan
January 30, 2026
Leaked Intel Core Ultra 7 356H Benchmark Scores Reveal Middling Gains
January 30, 2026
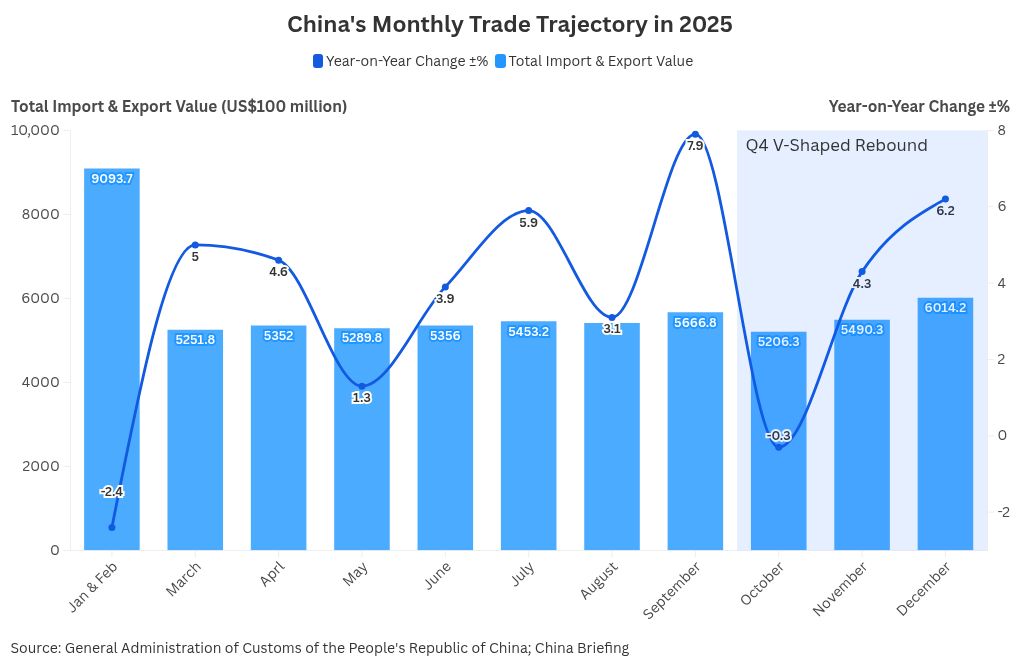
Trade Resilience and Structural Shifts
January 30, 2026