Qaasid News
Download Our App
Latest News from Pakistan
Pitbull to Headline Capital One Music Stage at Allstate Championship Tailgate
December 18, 2025
Breast Cancer: Slowing the growth of drug-resistant tumors
December 18, 2025
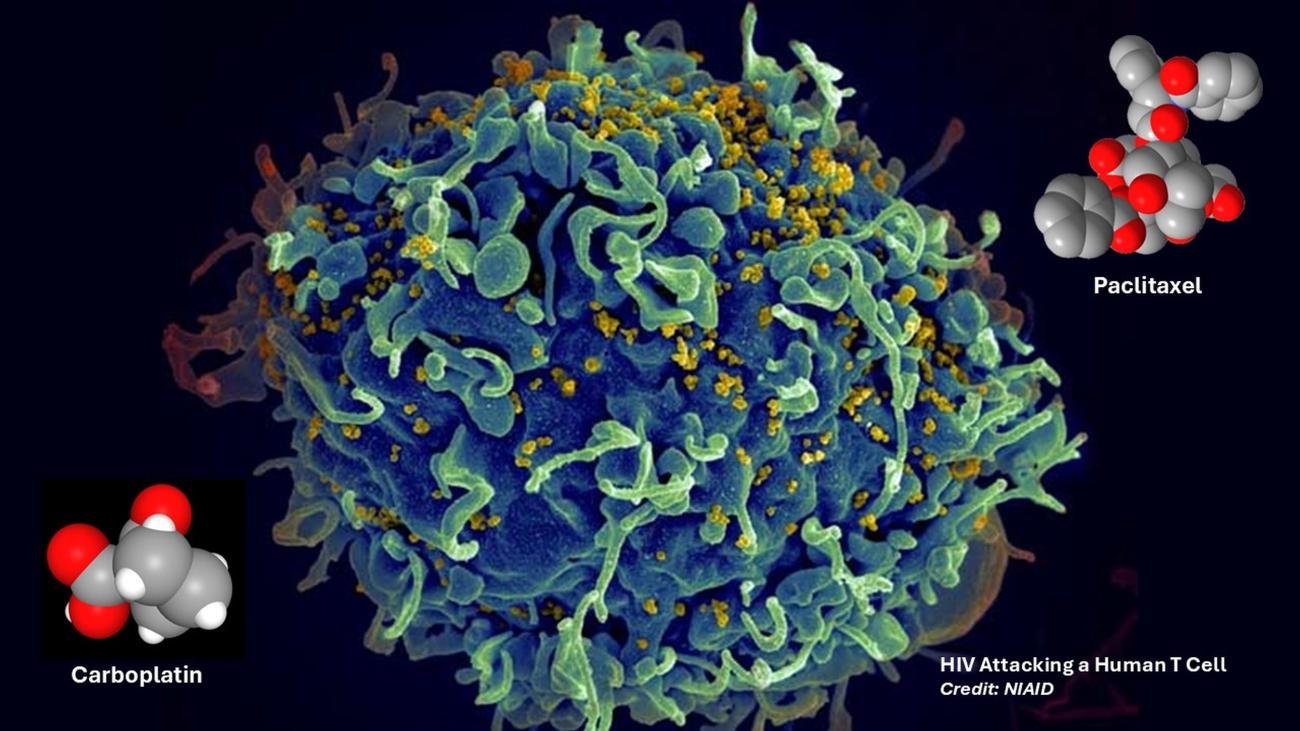
Patient sees dramatic drop in HIV-infected immune cells after cancer treatment
December 18, 2025
SCETV produces new short film profiling award-winning comic artist Sanford Greene for “HBCU Week NOW” | Stories | December 18, 2025
December 18, 2025
GM Announces 2025 full-year and Q4 earnings conference call details
December 18, 2025
Saskatchewan Exports Have Global Reach | News and Media
December 18, 2025
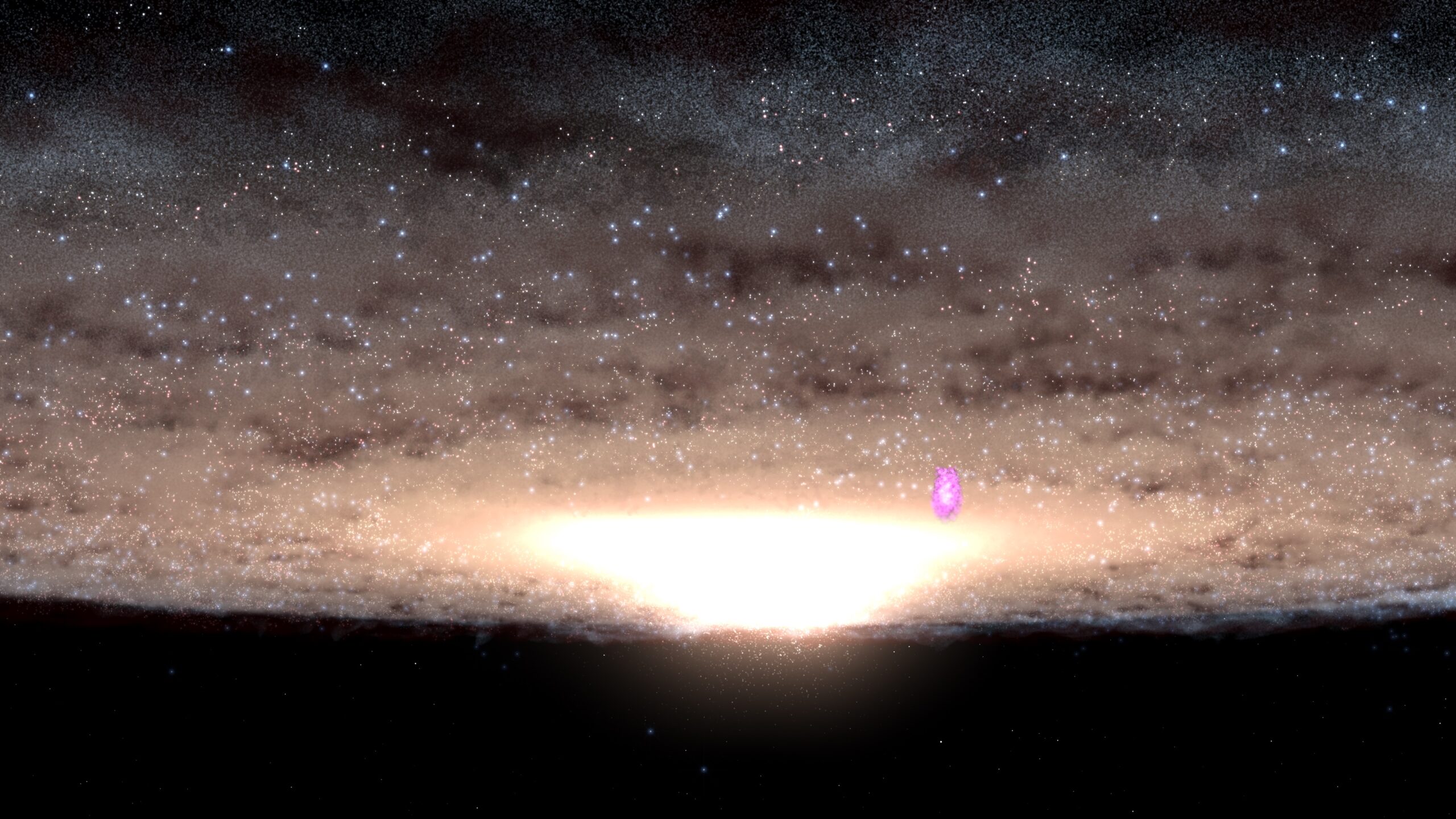
NASA SVS | NASA’s Fermi Spots Young Star Cluster Blowing Gamma-Ray Bubbles
December 18, 2025
Spray-on Antibacterial Coating Offers New Protection for Plants Against Disease and Drought
December 18, 2025
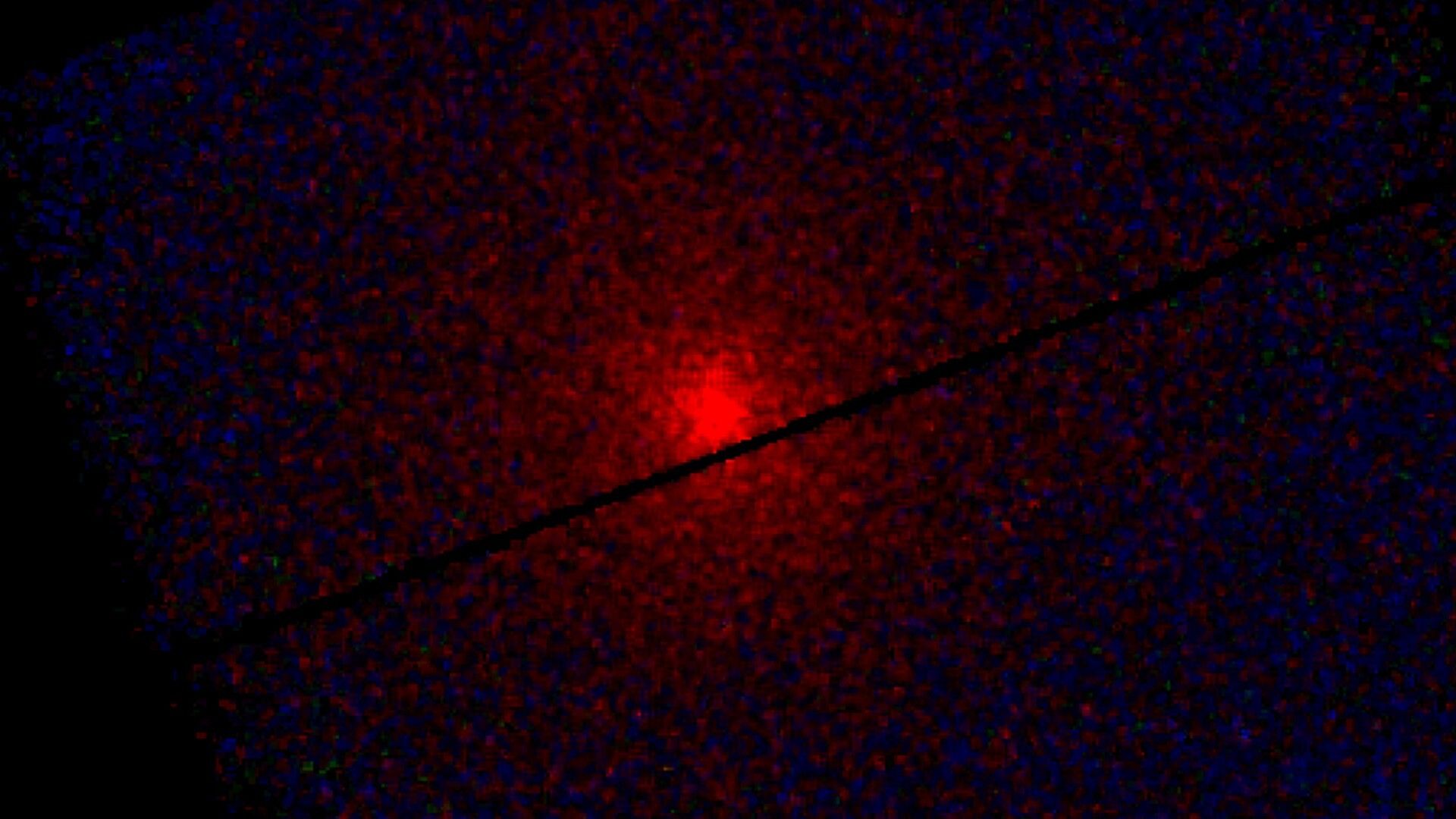
Scientists detect X-ray glow from interstellar comet 3I/ATLAS extending 250,000 miles into space
December 18, 2025
The Planetary Society’s 2025 book club review
December 18, 2025