Qaasid News
Download Our App
Latest News from Pakistan
Rapper Jeezy celebrates 20 years of ‘Thug Motivation 101’ with a 101-piece backing orchestra : NPR
December 14, 2025
Punjab Sahulat Bazar Authority earns Int’l certifications – RADIO PAKISTAN
December 14, 2025
Vitexin induces apoptosis and enhances daunorubicin efficacy in acute leukemia via modulation of the HIF-1α/Bcl-2/caspase-3 pathway
December 14, 2025
How Social Media Shapes Children’s Attention Over Time
December 14, 2025
ICYMI: Highlights From AACR 2025
December 14, 2025
Nanit Home Display Review: A Transformative Tablet
December 14, 2025
Bluey’s Quest for the Gold Pen: after some misfires we finally have the first good Bluey video game | Games
December 14, 2025
Little Foot hominin fossil may be new species of human ancestor | Evolution
December 14, 2025
I’m finally beginning to trust Microsoft’s handheld Xbox Allys
December 14, 2025
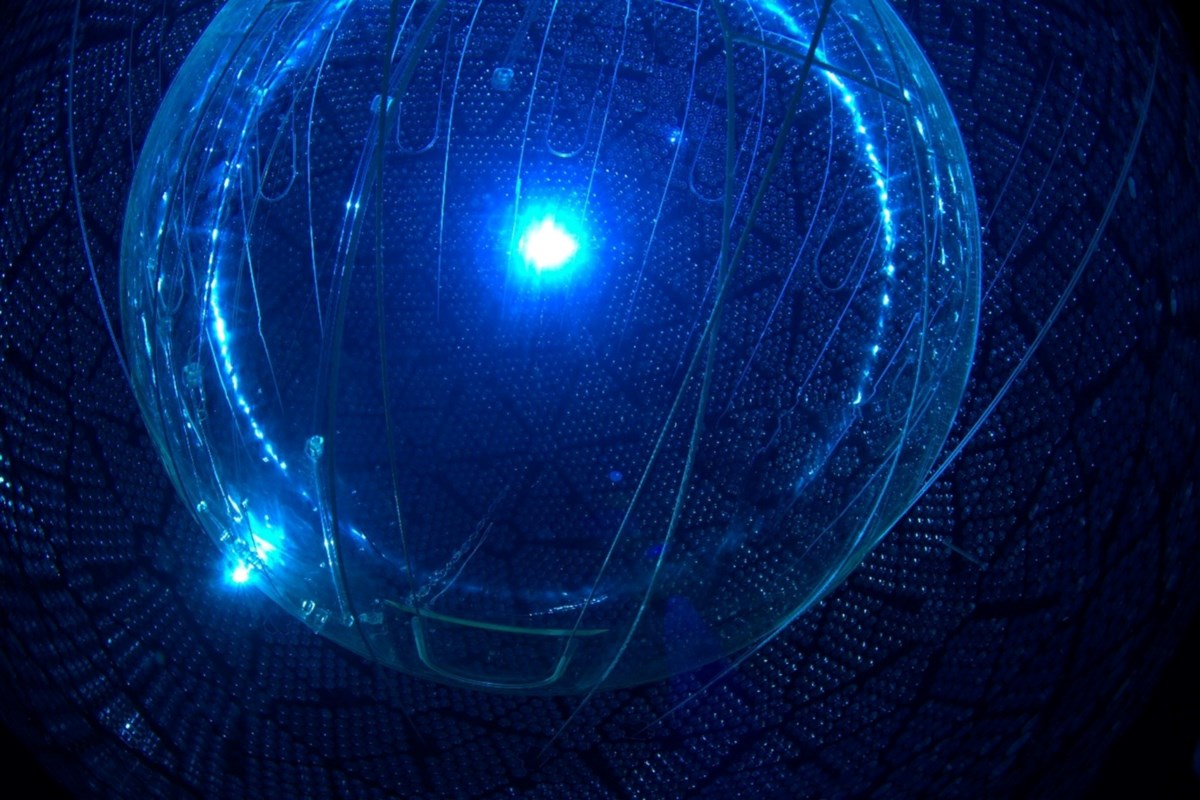
Oxford and SNOLAB scientists detect rare solar neutrino interaction
December 14, 2025