Qaasid News
Download Our App
Latest News from Pakistan
Access Denied
February 6, 2026
Lunar New Year concert highlights Zheng and Qin traditions | MSUToday
February 6, 2026
Climate activist group files second lawsuit against Sweden
February 6, 2026
A star is born: Israeli team detects stellar-creation particles 400 light-years away
February 6, 2026
‘Dracula’ Finds New Life in a Sexy Reimagining by Luc Besson – KQED
February 6, 2026
U.S. and Iran hold nuclear talks amid threats of regional war – The Washington Post
February 6, 2026
Andrew Mountbatten-Windsor’s friendship with a child sex offender turns his future murkier
February 6, 2026
Actor Timothy Busfield indicted in New Mexico on child sex abuse charges | New Mexico
February 6, 2026
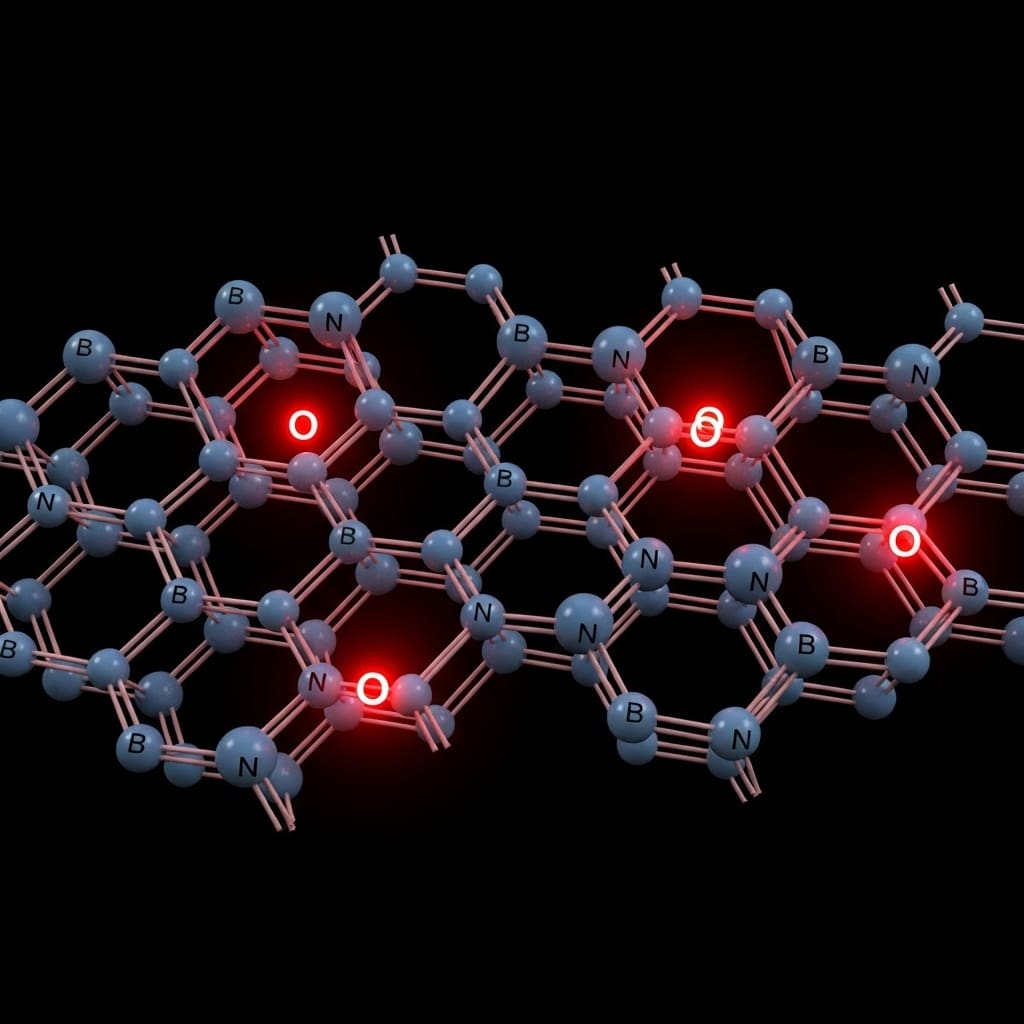
Oxygen Flaws Unlock The Source Of Bright Light In Hexagonal Boron Nitride
February 6, 2026
First Plenary at MASCC26: Maximizing Access to Supportive Care for All – MASCC
February 6, 2026