Qaasid News
Download Our App
Latest News from Pakistan
What causes chronic pain? New study identifies key culprit in the brain – Medical Xpress
January 28, 2026
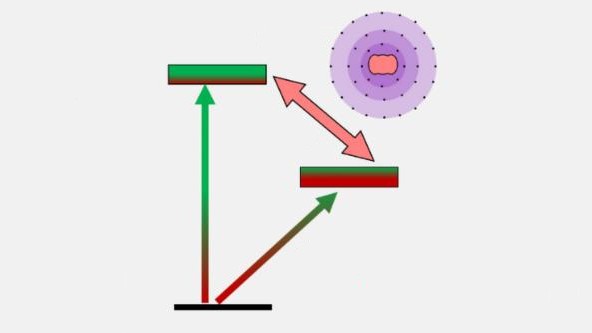
Ion-clock transition could benefit quantum computing and nuclear physics – Physics World
January 28, 2026
Built to Unleash AMD Ryzen X3D Processors: GIGABYTE AI-Powered X870E AORUS XTREME X3D AI TOP Motherboard Now Available – PR Newswire APAC – PR Newswire Asia
January 28, 2026
Threat of US-Iran war escalates as Trump warns time running out for deal | Iran
January 28, 2026
Ex-Spandau Ballet singer found guilty of rape – BBC
January 28, 2026
India trade deal cements EU’s voice in ‘multipolar world’, Costa tells Euronews
January 28, 2026
Lawmakers condemn ‘disgusting’ attack on Ilhan Omar at Minneapolis town hall | Ilhan Omar
January 28, 2026
Putin is hosting Syria’s interim leader for talks, with Russian military bases on the agenda
January 28, 2026
The infant universe's 'primordial soup' was actually soupy, study finds – Phys.org
January 28, 2026
Green Assist: transforming agricultural waste into cosmetics and food
January 28, 2026