Qaasid News
Download Our App
Latest News from Pakistan
Geminid meteor shower: where to watch Australia’s biggest shooting star show this weekend | Meteors
December 10, 2025
Jesus ‘I’m more than ready’ | Interview | News
December 10, 2025
Vue cinema staff go on strike in Glasgow over work conditions
December 10, 2025
Samsung Electronics and KT Corporation Successfully Validate AI-RAN on Commercial Networks, Accelerating 6G Development – Samsung Global Newsroom
December 10, 2025
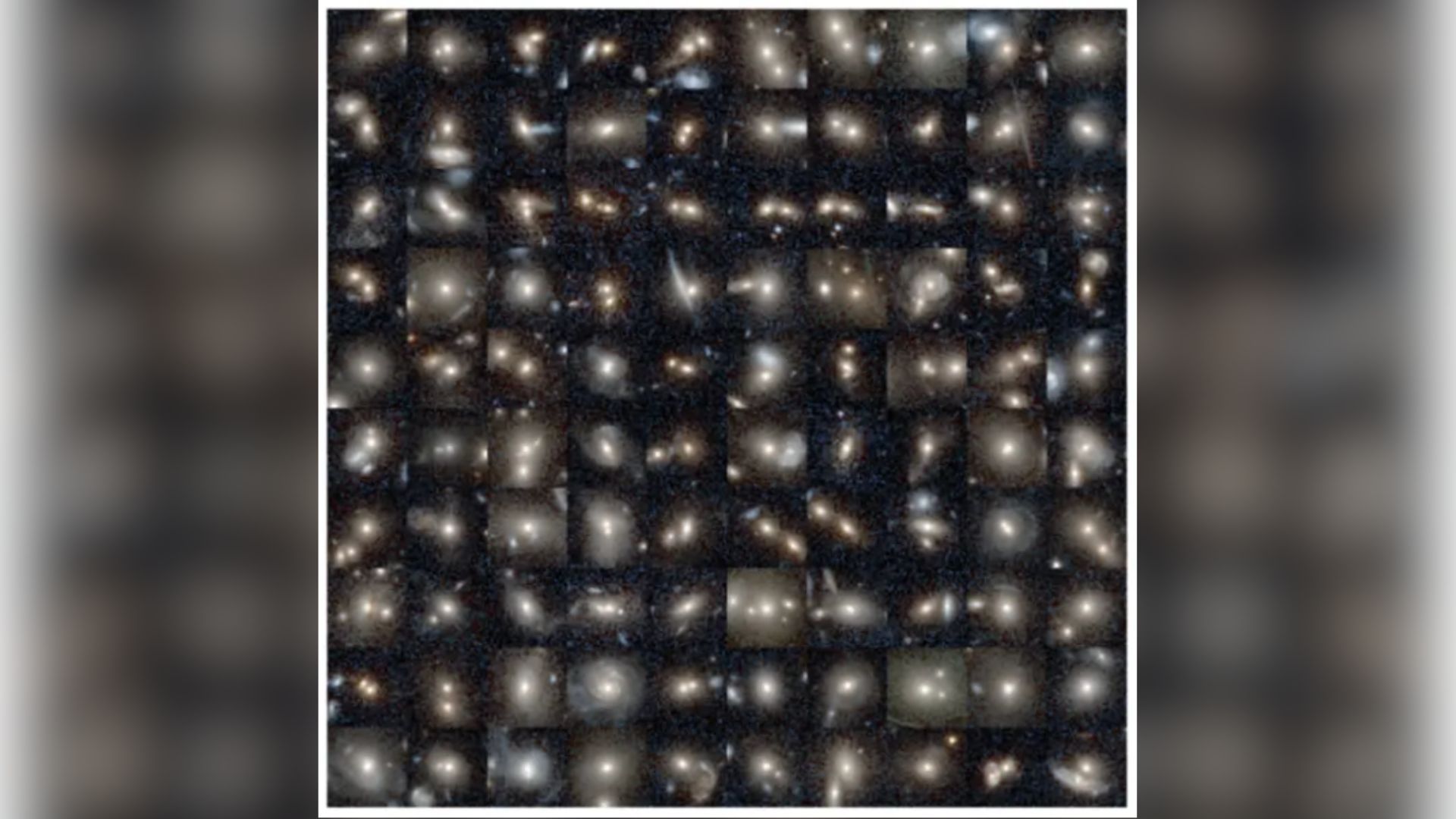
How do you activate a supermassive black hole? A galaxy merger should do the trick
December 10, 2025
This 100TB encrypted cloud storage lifetime subscription is now 90% off
December 10, 2025
WTA Tour signs landmark Mercedes sponsorship deal as ATP commercial merger moves closer
December 10, 2025
Trump administration says it seized oil tanker off Venezuela coast | Donald Trump News
December 10, 2025
Even in Wintry Weather, Taylor Swift Remains Committed to the Miniskirt
December 10, 2025
Chefs from MICHELIN Restaurants Collaborate Live on Gaggenau’s Expressive Series
December 10, 2025