Qaasid News
Download Our App
Latest News from Pakistan
16th EU-India Summit: advancing our Strategic Partnership across trade and defence – European Commission
January 27, 2026
WHO EMRO – WHO and CAF promote healthy lifestyles at the U-15 African Schools Football Championship
January 27, 2026
Amy DuBois Barnett Explores Ambition, Identity And Power In Debut Novel ‘If I Ruled The World’
January 27, 2026
Organic growth and solid cash flow to end the year
January 27, 2026
SCIRP Open Access
January 27, 2026
Pakistan ready to play role in shaping global labour market: Salik – RADIO PAKISTAN
January 27, 2026
Samsung Unveils Exclusive Galaxy Z Flip7 Olympic Edition, Supporting Athletes’ Entire Milano Cortina 2026 Journey – Samsung Global Newsroom
January 27, 2026
Xi says China, Finland should uphold international system, advance multipolar order – Reuters
January 27, 2026
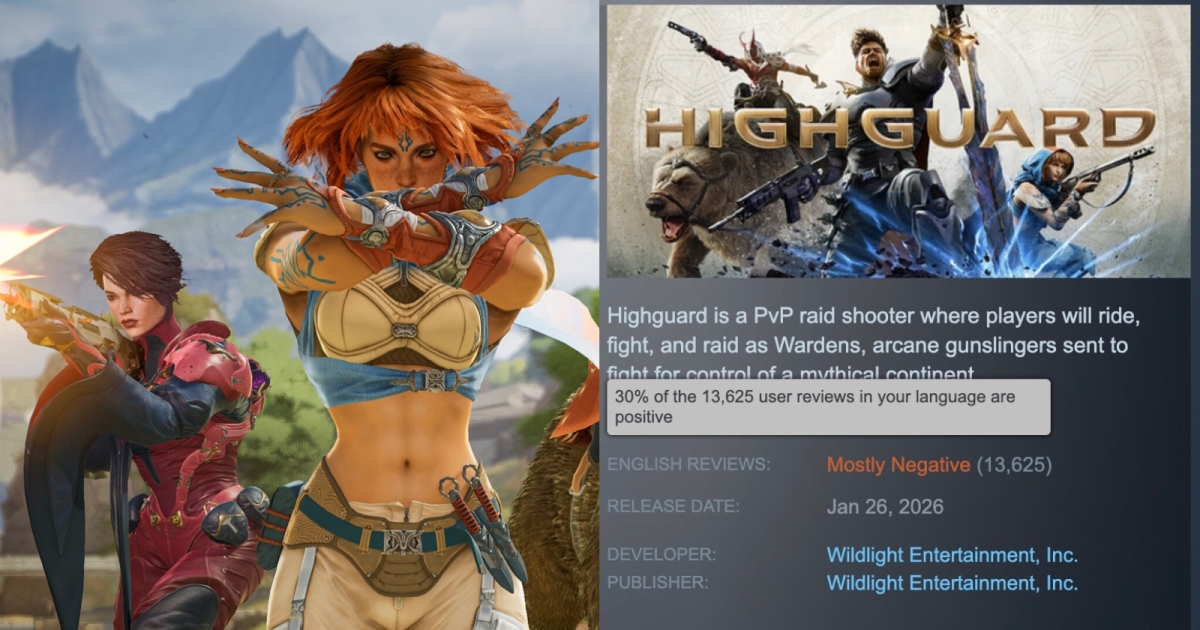
Highguard, 2026’s First Contentious Title, Performs Poorly at Launch
January 27, 2026
Govt endeavouring to improve quality of education: Wajiha – RADIO PAKISTAN
January 27, 2026