Qaasid News
Download Our App
Latest News from Pakistan
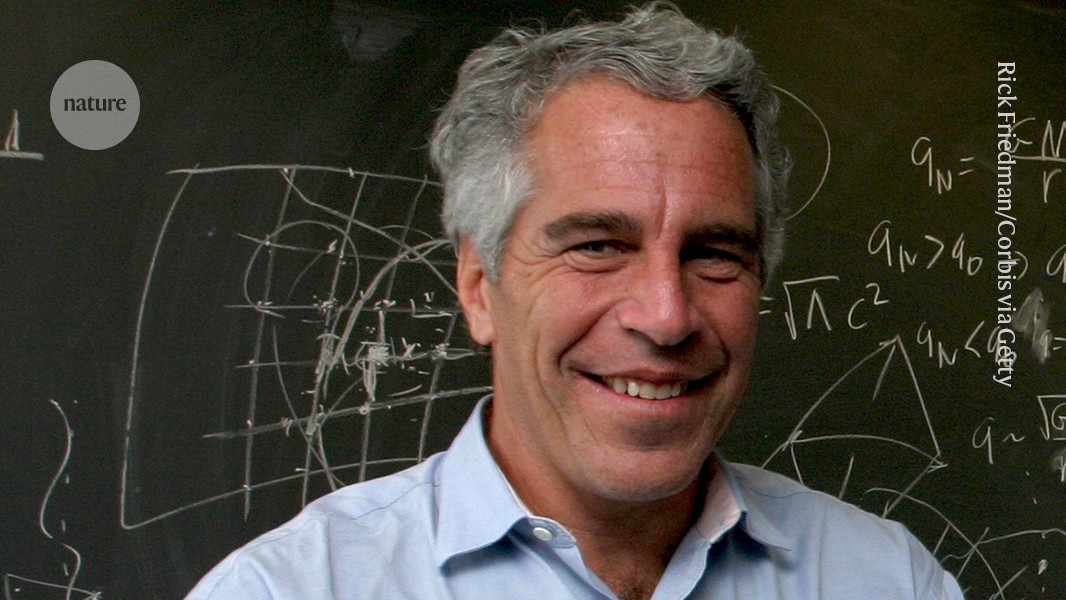
Epstein files reveal deeper ties to scientists than previously known
February 6, 2026
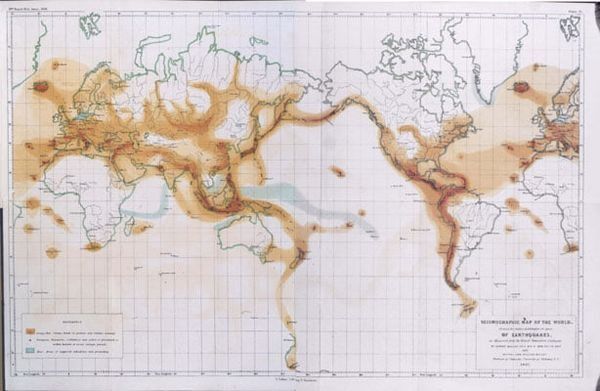
First map of rare mantle earthquakes compiled
February 6, 2026
Guterres welcomes resumption of Iran-US talks – news.un.org
February 6, 2026
Earn‑out acceleration after closing: Lessons from Project Freeway v. ABC Technologies | Canada | Global law firm
February 6, 2026
Queen’s image on Australian commemorative coins likened to Shrek | Monarchy
February 6, 2026
Access Denied
February 6, 2026
Access Denied
February 6, 2026
Access Denied
February 6, 2026
Stocks making the biggest moves midday: AMZN, CNC, RBLX
February 6, 2026
Iran, US hold talks in Oman as fears of war hang over region | News
February 6, 2026