Qaasid News
Download Our App
Latest News from Pakistan
Where silence is its own language
February 6, 2026
Probiotics For Cancer And Diabetes?
February 6, 2026
Global electricity demand is set to grow strongly to 2030, underscoring need for investments in grids and flexibility – News
February 6, 2026
A star is born: Israeli team detects stellar-creation particles 400 light-years away
February 6, 2026
Kashmir Solidarity Day observed at Embassy of Pakistan in Paris – RADIO PAKISTAN
February 6, 2026
Has Sindh Announced a Holiday for Schools Tomorrow?
February 6, 2026
Kuehne+Nagel opens new Container Freight Station to meet India’s growing trade needs
February 6, 2026
US and Iran set for further talks in Oman amid Trump’s military threats – live | Iran
February 6, 2026
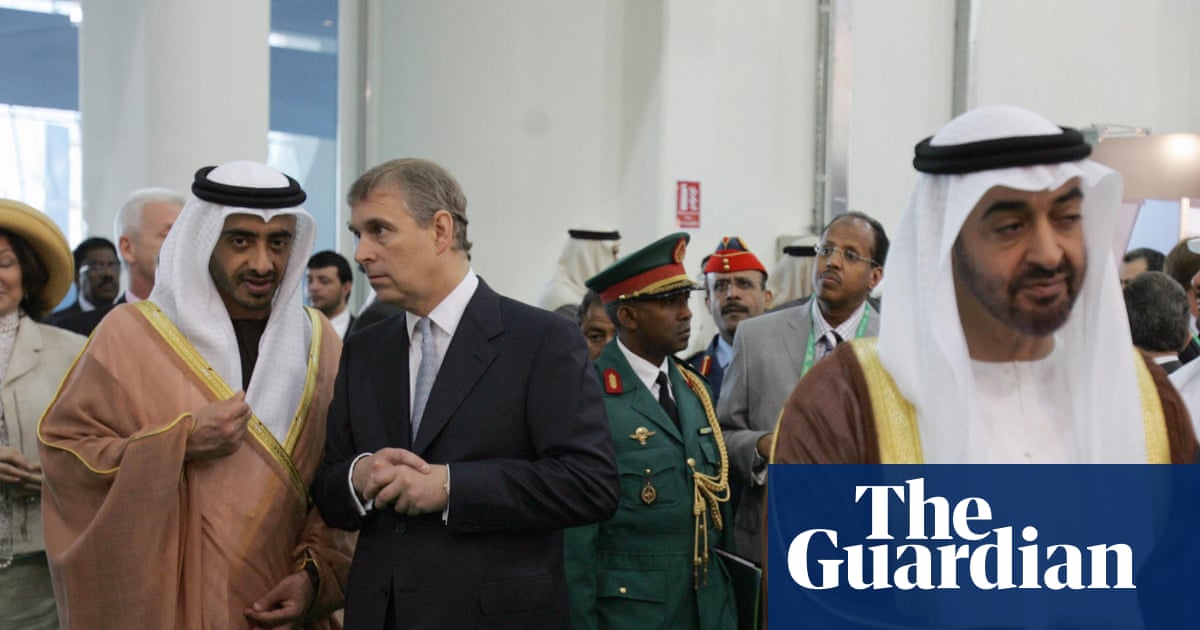
Andrew vouched for Epstein on state visit to UAE with queen in 2010 | Andrew Mountbatten-Windsor
February 6, 2026
Activists plan new, bigger flotilla to try to bring aid to Gaza – Arab News
February 6, 2026