Qaasid News
Download Our App
Latest News from Pakistan
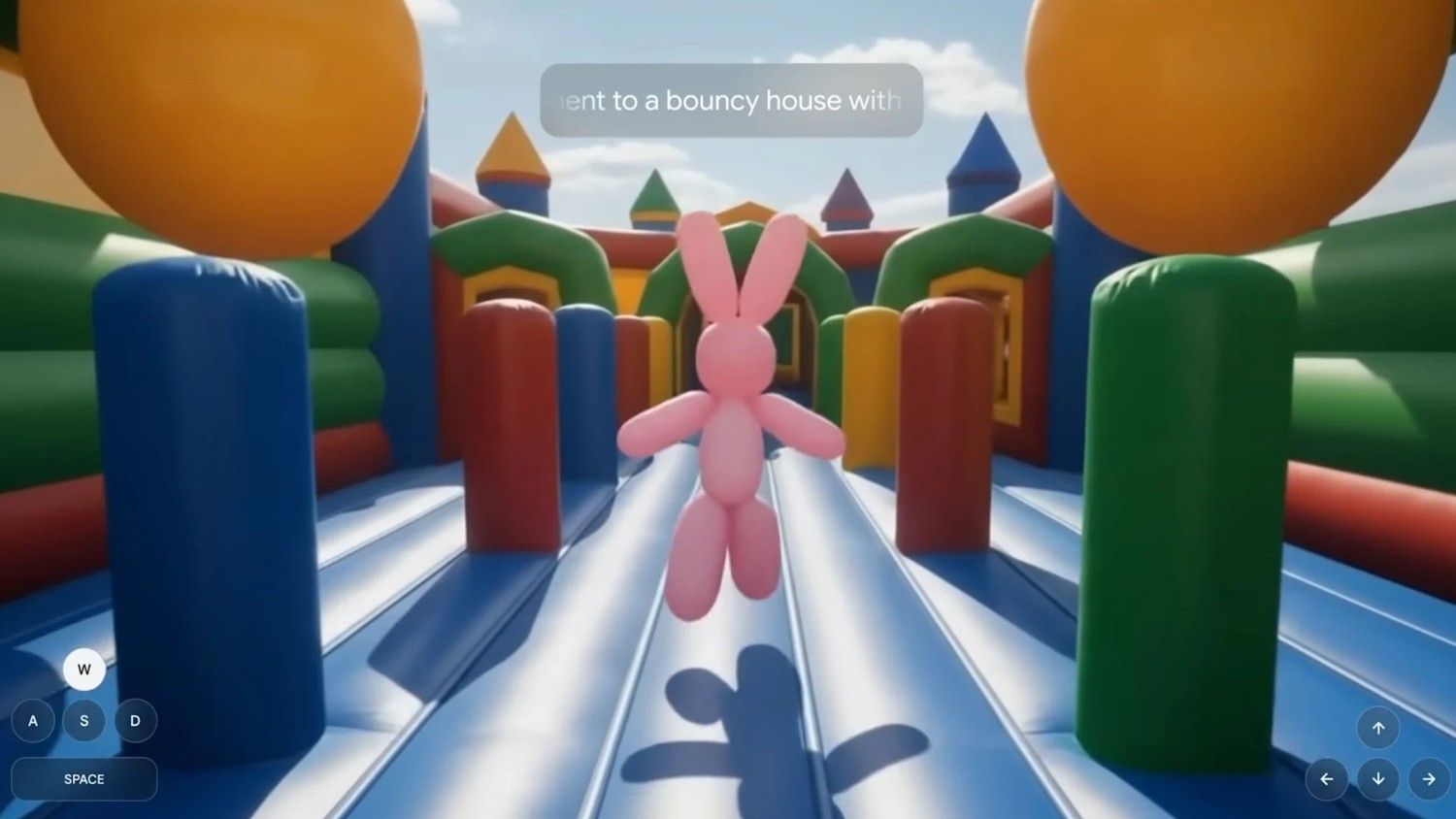
How Google’s new AI could change videogames forever – Fast Company Middle East
February 6, 2026
Kit Harington at 39: Rehab, fame, fatherhood and me – The Times
February 6, 2026
The Real Risks of the Saudi-UAE Feud
February 6, 2026
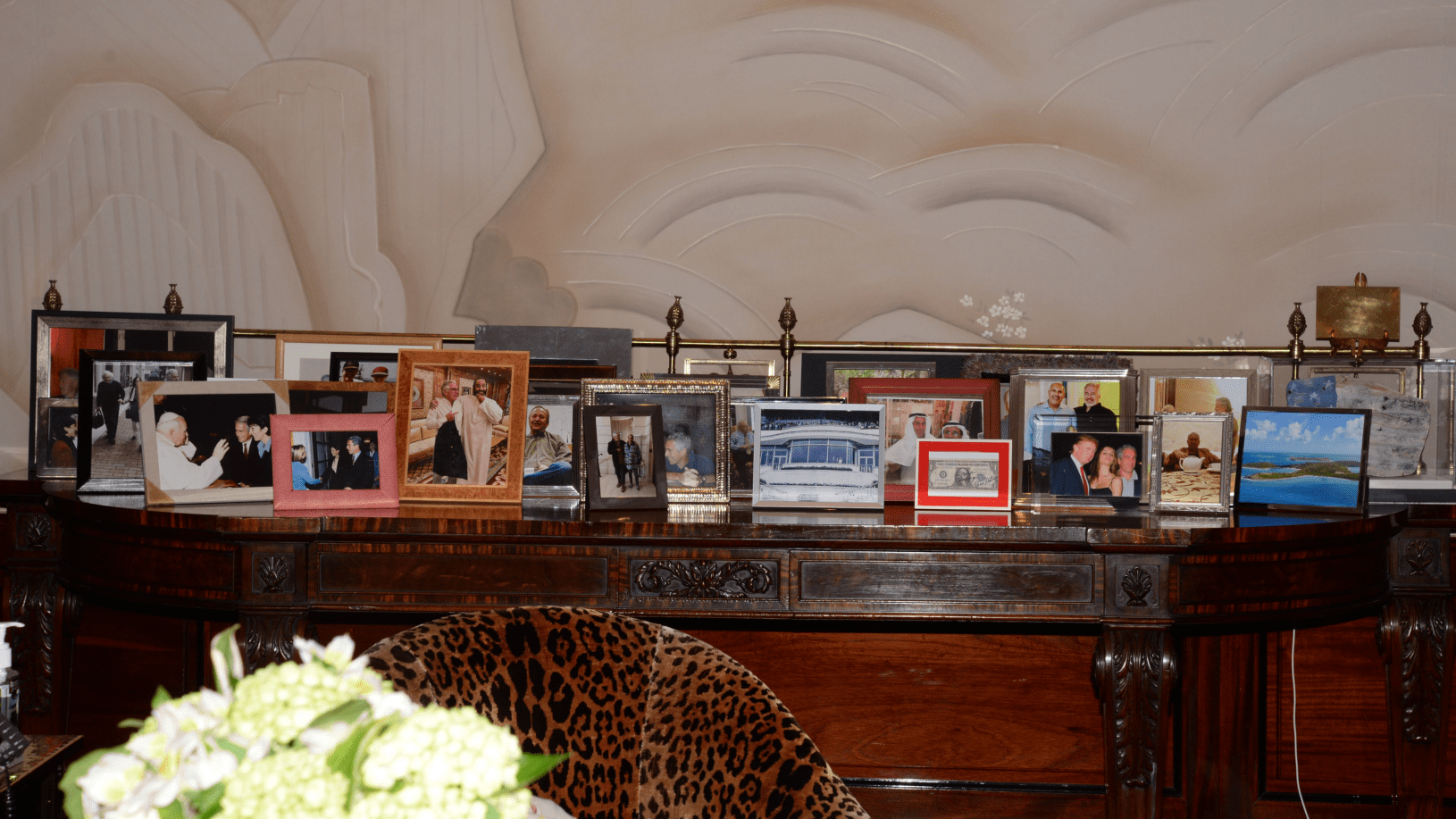
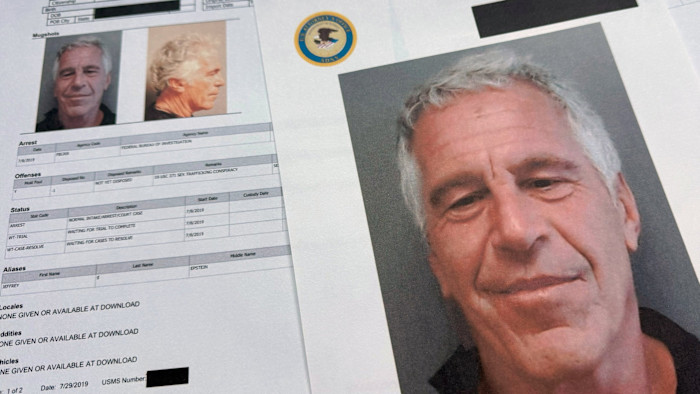
Inside Jeffrey Epstein’s social Ponzi scheme – Financial Times
February 6, 2026
How Jeffrey Epstein leveraged Wall Street
February 6, 2026
‘I’ve been advised not to say certain things’: The Secret Agent makers on Oscars, dictators and death threats | Film
February 6, 2026
Australia’s 2026 Aacta awards red carpet – in pictures – The Guardian
February 6, 2026
Some early life forms may have breathed oxygen well before it filled the atmosphere | MIT News
February 6, 2026
Today’s Hurdle hints and answers for February 6, 2026
February 6, 2026
Baker McKenzie Advises Flowserve on USD 490M Strategic Acquisition of Trillium Flow Technologies’ Valves Division | Newsroom
February 6, 2026