Qaasid News
Download Our App
Latest News from Pakistan
Chinese TV brands projected to reach 60% share in Japan market · TechNode
February 6, 2026
Iran and US set for talks in Oman over nuclear program
February 6, 2026
Smartwatch data may help detect opioid misuse risk
February 6, 2026
SCIRP Open Access
February 6, 2026
Venolymphatic Malformation Presenting as a Low-Flow Vascular Anomaly: A Case Report
February 6, 2026
Azerbaijan urged to free detained women journalists
February 6, 2026
Pakistan embassy in Beijing commemorates Kashmir Solidarity Day – Business Recorder
February 6, 2026
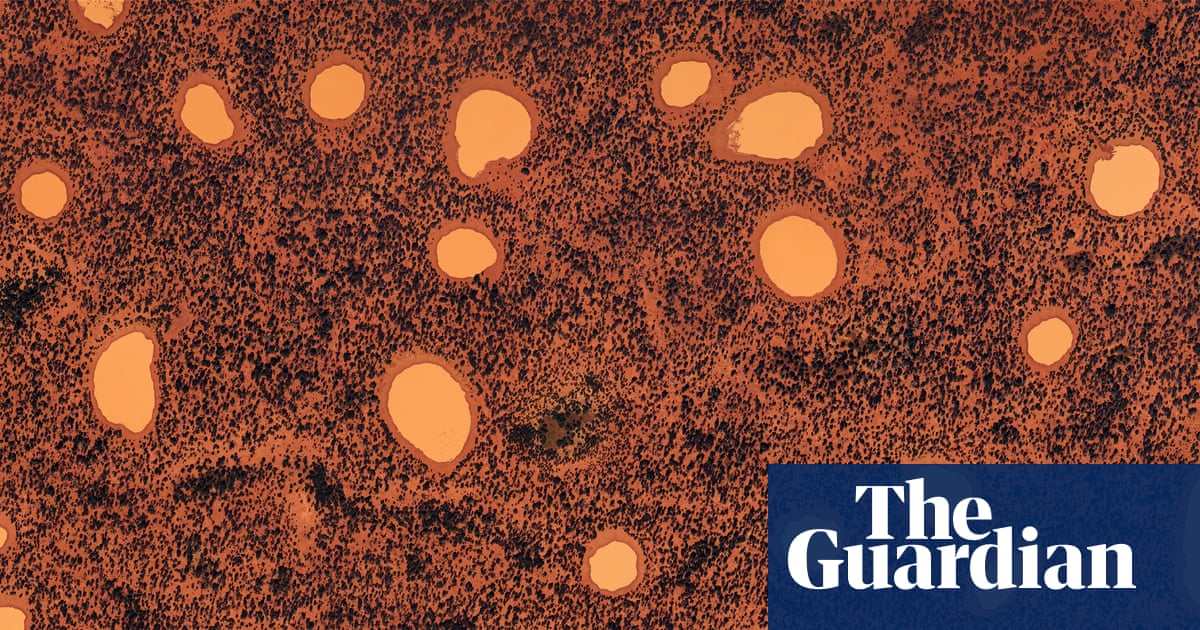
Beautifully strange: Australian landscapes photographed from the sky – in pictures | Australian art
February 6, 2026
PTI, TTAP ‘will not compromise’ on Imran’s health
February 6, 2026
Paid sick leave emerges as key workplace support for frontline workers, new study shows
February 6, 2026