Qaasid News
Download Our App
Latest News from Pakistan
Duffy takes four as New Zealand crush West Indies to seal T20 series
November 13, 2025
Access Denied
November 13, 2025
One cup of coffee a day may reduce the risk of irregular heartbeat, finds a study
November 13, 2025
Duffy takes four as New Zealand crush West Indies to seal T20 series
November 13, 2025
Trump signs spending bill to end longest shutdown in US history
November 13, 2025
South Park Tackles Deepfakes as Manipulated Videos Hit the Town
November 13, 2025
How Pacific nations plan to go from spending up to 25% of GDP on fossil fuels to running on 100% renewables
November 13, 2025
Samsung Galaxy A37 is on its way, test firmware shows
November 13, 2025
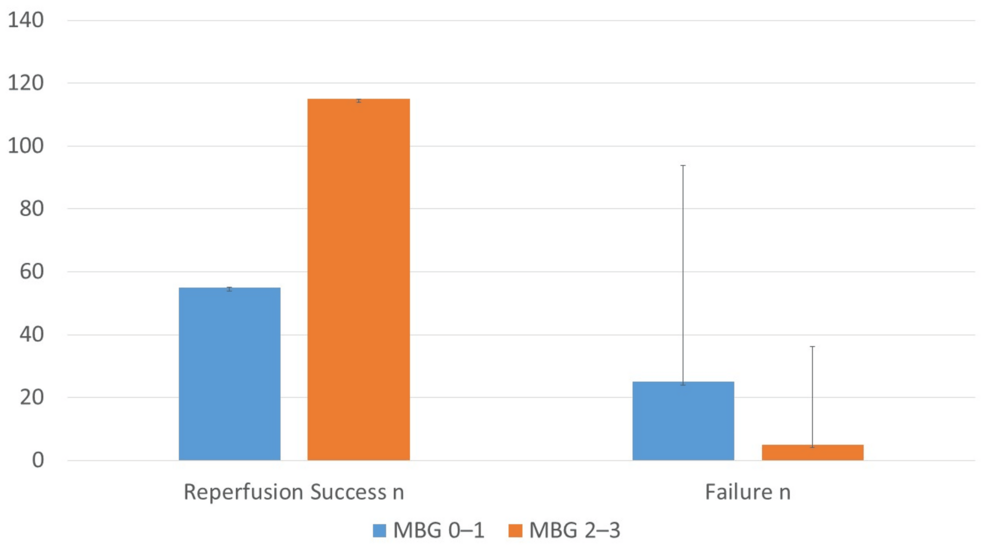
Prognostic Value of Myocardial Blush Grade in Patients With ST-Segment Elevation Myocardial Infarction (STEMI) Undergoing Primary Percutaneous Coronary Intervention (PCI): Association With Reperfusion Success and In-Hospital Outcomes
November 13, 2025
TRIMTECH Therapeutics appoints Dr Mike Hutton to Scientific Advisory Board
November 13, 2025