Qaasid News
Download Our App
Latest News from Pakistan
UK study to examine effects of restricting social media for children | Social media
January 20, 2026
Opera is not dying – but it needs a second act for the streaming era
January 20, 2026
AO 2026: Wawrinka writing final chapter with pure joy – Roland-Garros 2026
January 20, 2026
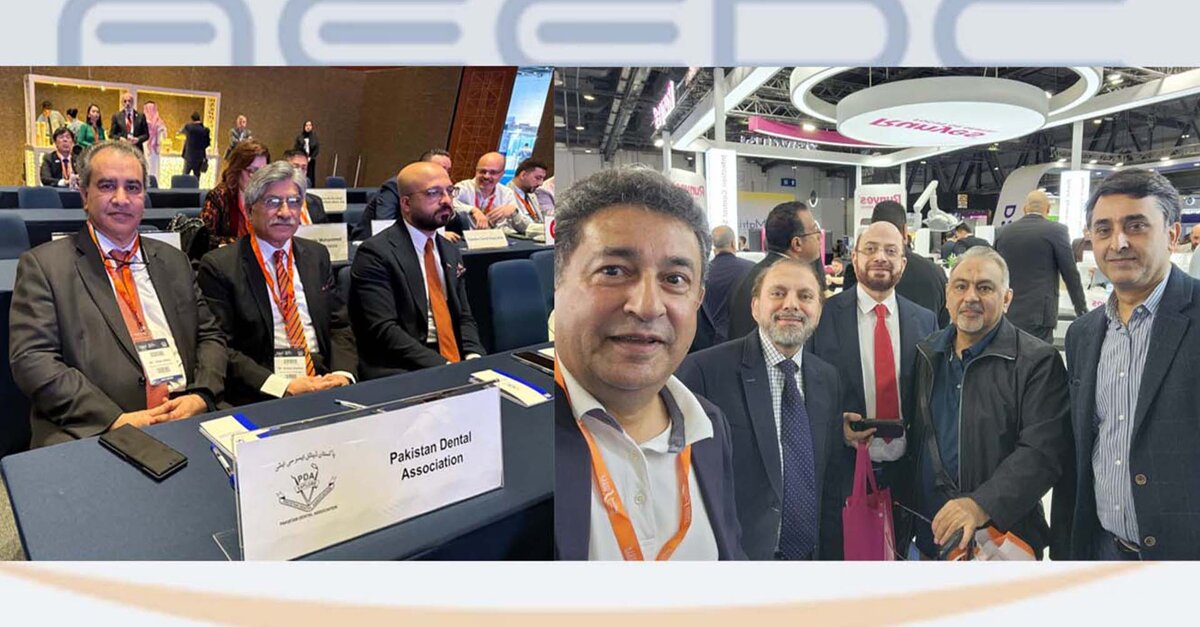
DT News – Pakistan – AEEDC Dubai 2026: Pakistan’s Strong Presence at the Global Dental Summit
January 20, 2026
India flights barred as Pakistan renews airspace closure for another month
January 20, 2026
FUJIFILM GFX ETERNA 55 Filmmaking Camera Joins Fleet of IMAX®-Certified Digital Cameras
January 20, 2026
Israel bulldozes UN agency for Palestinian refugees
January 20, 2026
Julie Béna’s Nocturnal Carnival – ArtReview
January 20, 2026
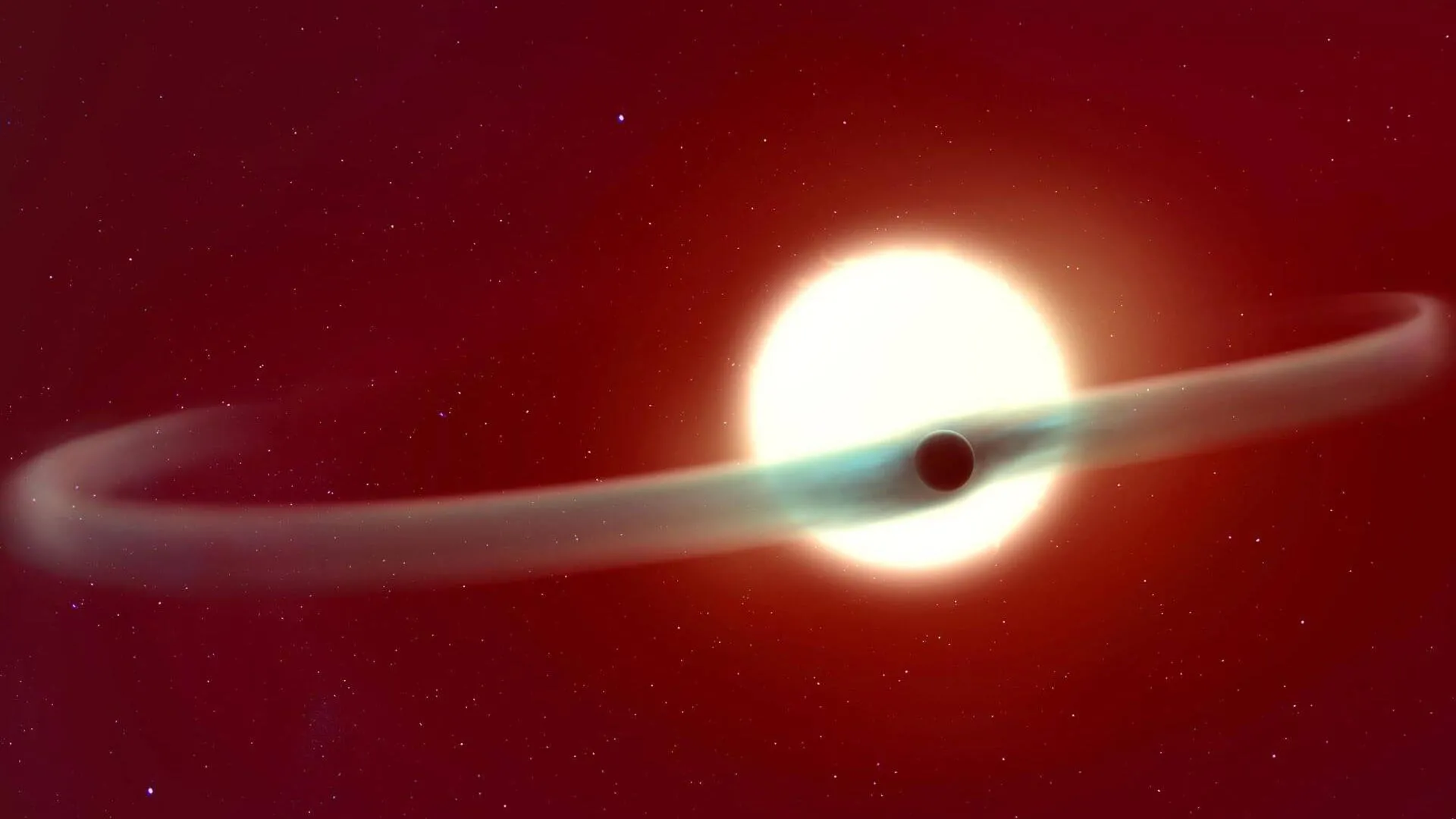
James Webb catches an exoplanet losing its atmosphere in real time
January 20, 2026
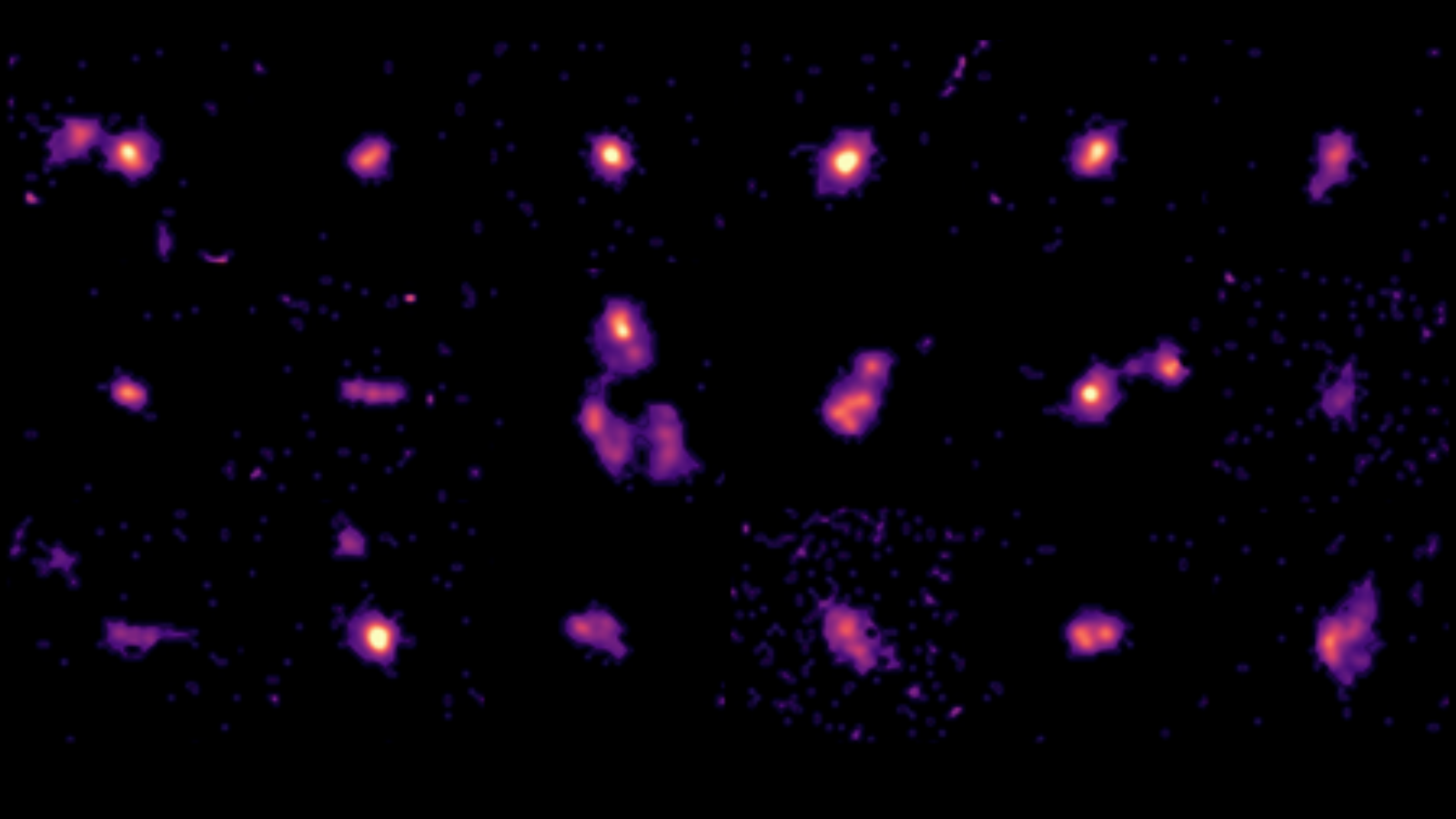
James Webb Space Telescope discovers young galaxies age rapidly: ‘It’s like seeing 2-year-old children act like teenagers’
January 20, 2026