Qaasid News
Download Our App
Latest News from Pakistan
Two high-speed trains collide in Spain, police sources say 21 people killed
January 19, 2026
Sudan: Atrocities ‘repeated town by town’, ICC prosecutor tells UN Security Council – UN News
January 19, 2026
NBA Fantasy: Power Rankings entering Week 14
January 19, 2026
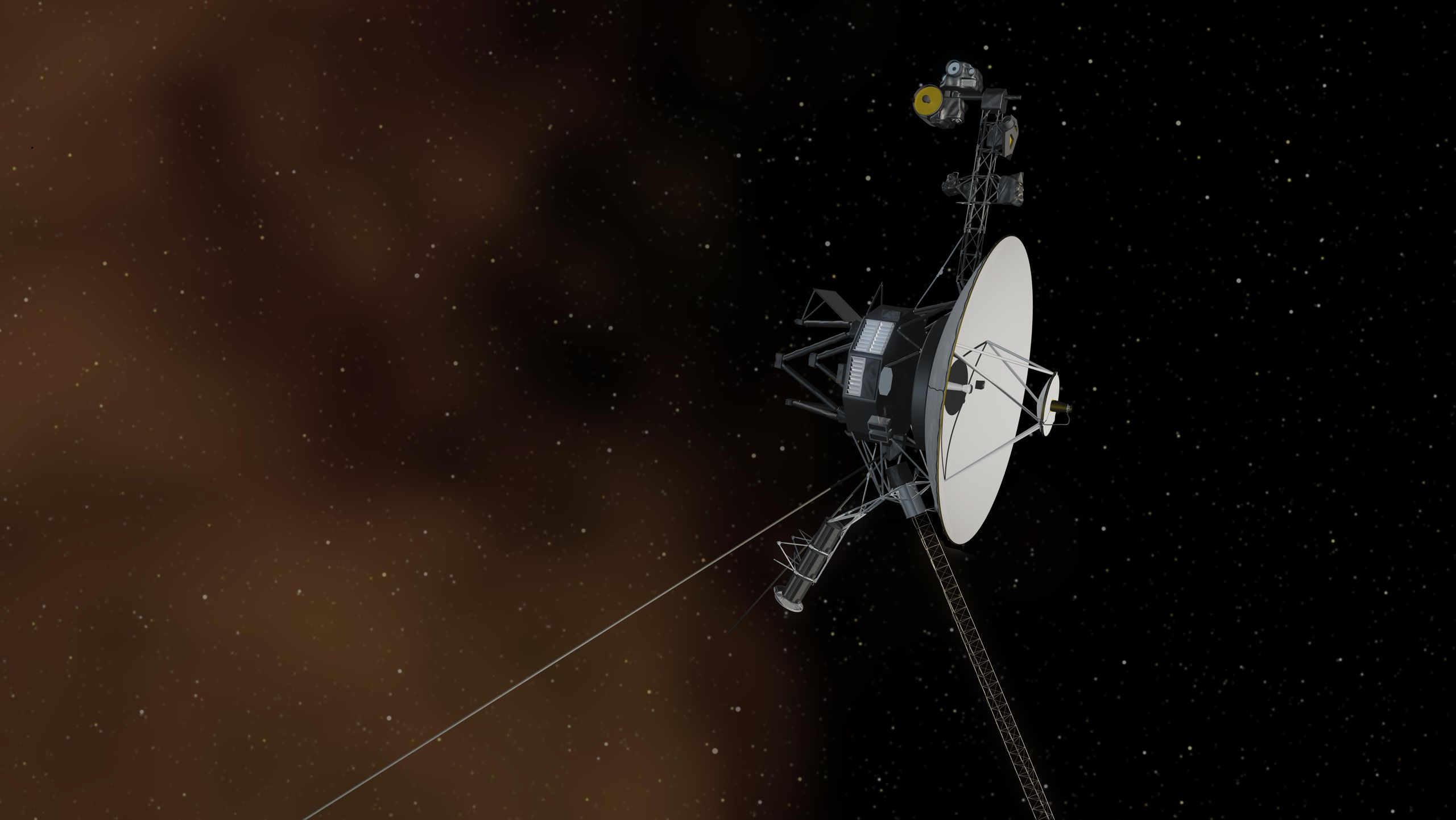
How to find 4 legendary spacecraft in January’s night sky
January 19, 2026
Apple led global smartphone market in 2025, overtaking Samsung at the post
January 19, 2026
DNV: Can MENA Renewable Energy Supply Keep Up With Demand? – Sustainability Magazine
January 19, 2026
Incretin-Based Drugs May Reduce Risk of Dementia in Patients With Type 2 Diabetes
January 19, 2026
Pakistan-Saudi defence pact expansion to be decided jointly: defence minister
January 19, 2026
Jermelle Simon on How ‘The Upshaws’ Stopped Him Fearing His Sexuality
January 19, 2026
Imam sentenced for conducting child marriage in UK legal first | UK | News
January 19, 2026