Qaasid News
Download Our App
Latest News from Pakistan
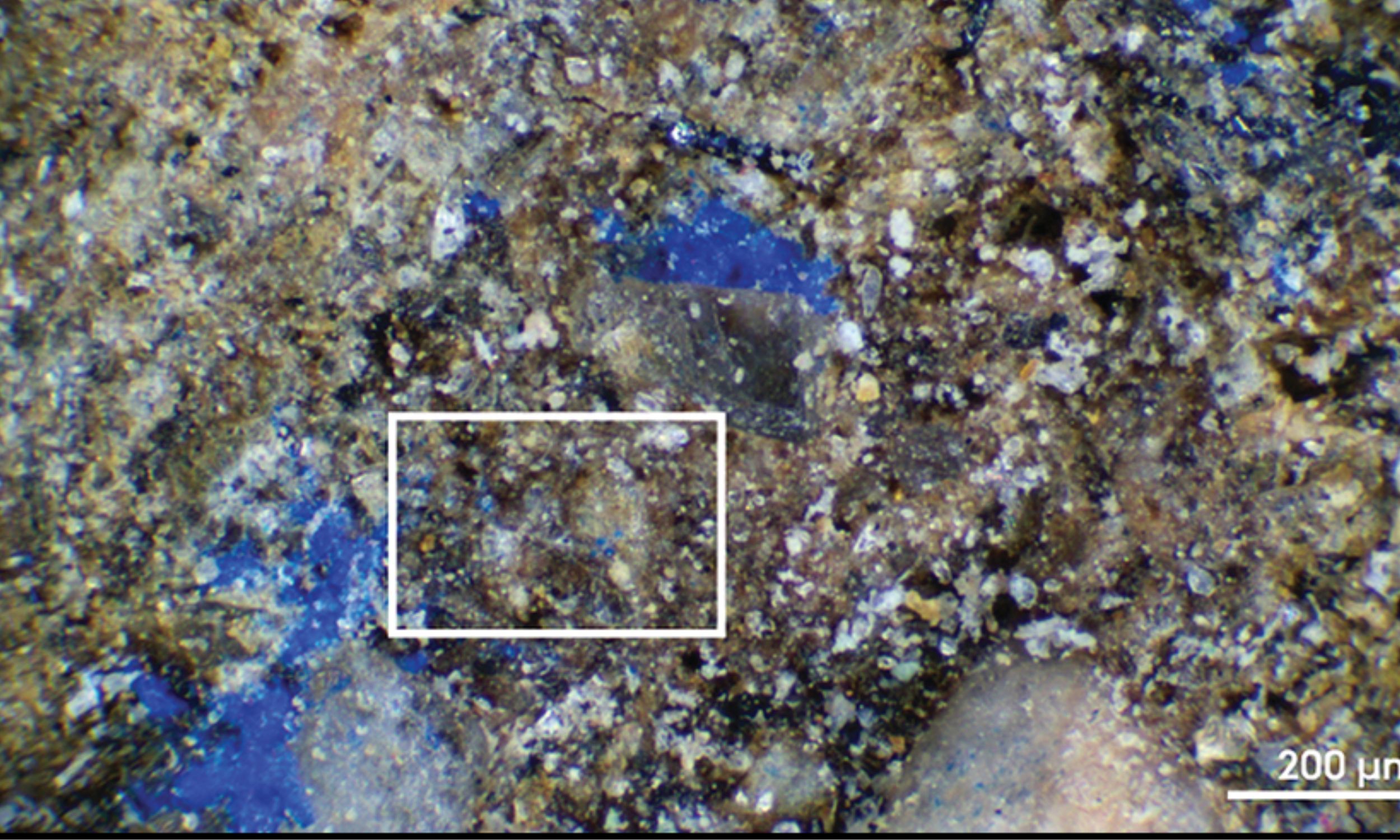
Forgotten museum object holds Europe’s oldest blue pigment
February 8, 2026
Mikaela Shiffrin embraces “pressure” ahead of her fourth Olympics
February 8, 2026
Apple’s thinnest iPhone sees sales triple after multiple price drops
February 8, 2026
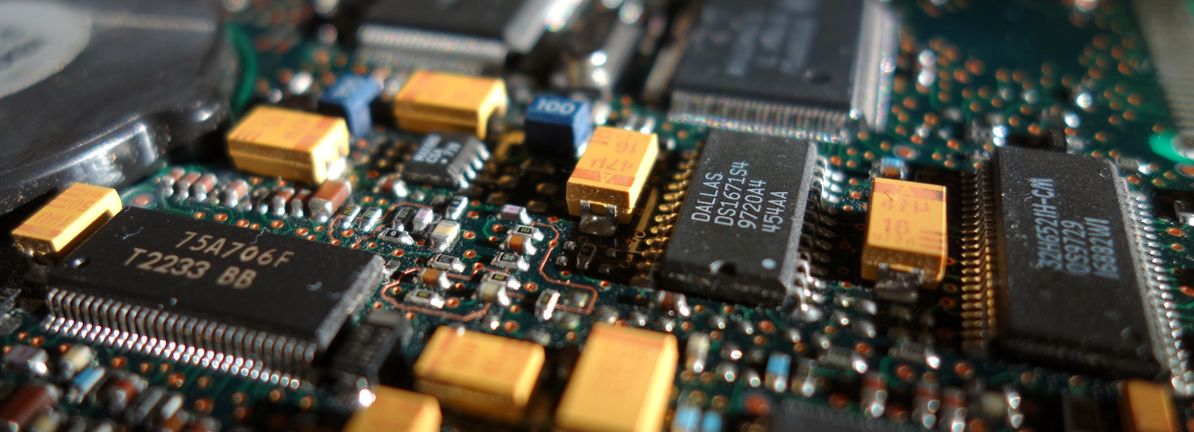
Monolithic Power Systems (MPWR) Is Up 9.4% After Dividend Hike And Revenue Guidance Update
February 8, 2026
Pakistan’s Strategic Posture amid Escalating Iran-US Tensions
February 7, 2026
Fossil crustaceans reveal ancient routes across the North Pacific
February 7, 2026
SpaceX Crew-12 will Study How Microgravity Affects the Human Body
February 7, 2026
Washington Post publisher Will Lewis abruptly resigns amid criticism of staff cuts | Washington Post
February 7, 2026
Marques Brownlee sparks controversy after YouTuber questions safety and long term risks of silicon carbon smartphone batteries
February 7, 2026
Kingdom Hearts remake and Kingdom Hearts 4 tipped for 2027 in new Square Enix leak
February 7, 2026