Qaasid News
Download Our App
Latest News from Pakistan
Goldman Sachs Initiates Workday (WDAY) at Neutral as Challenging Market Share Gains Temper AI Optimism
January 19, 2026
The 38-year-old made it 100 wins at the Australian Open to reach the second round of the 2026 Grand Slam in Melbourne.
January 19, 2026
Higher omega-3 blood levels linked to reduced early-onset dementia risk despite genetics
January 19, 2026
Saul Nash Men’s Fall 2026 Ready-to-Wear Runway, Fashion Show & Collection Review
January 19, 2026
Prosser: iPhone 18 Pro Dynamic Island Moving to Top-Left Corner
January 19, 2026
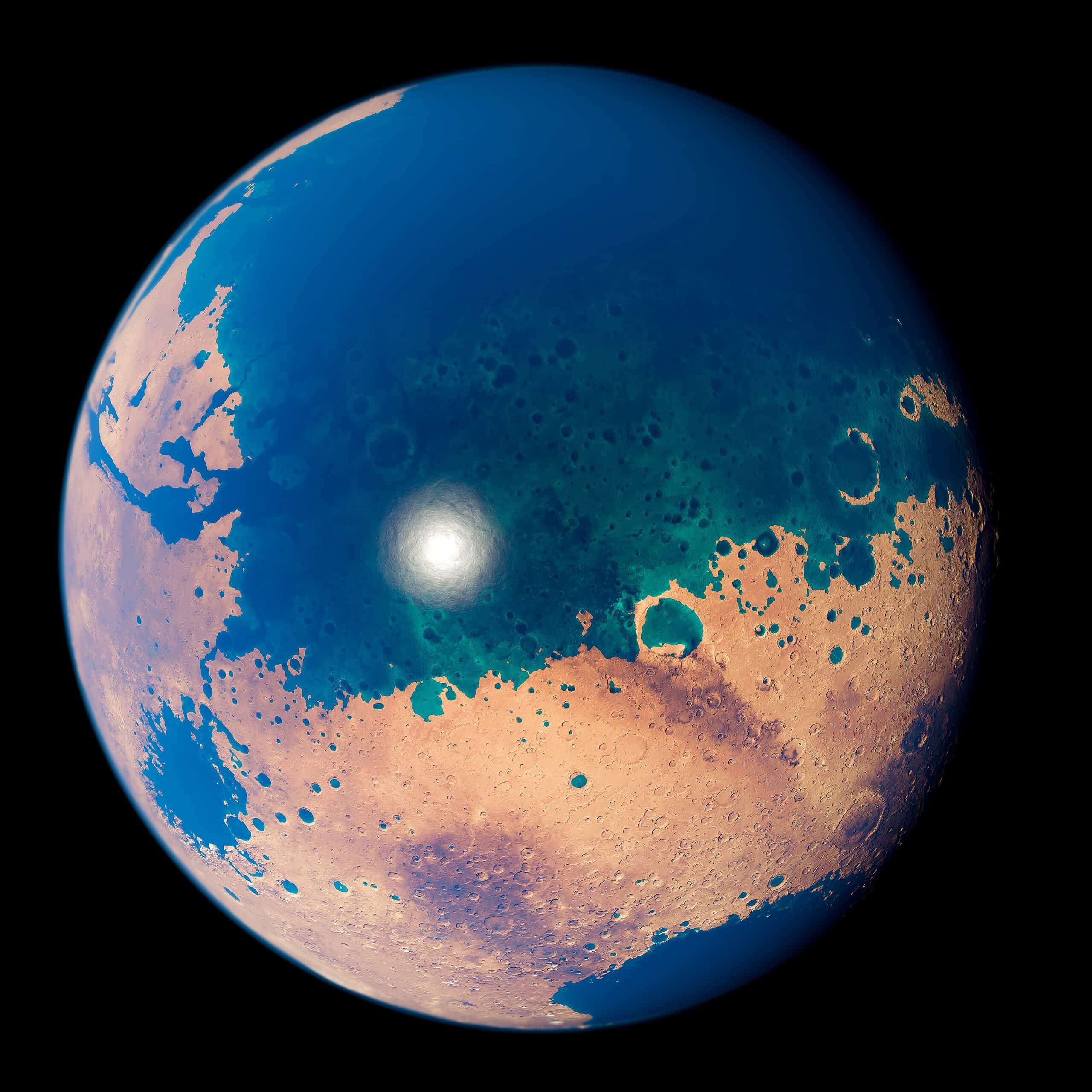
Deltas and Canyons on Mars Hint at Ocean That Covered Half the Planet
January 19, 2026
Kao Group hosts limited-time pop-up in Japan to showcase make-up brand Kate
January 19, 2026
Gold and silver prices hit high after tariff threat
January 19, 2026
Marti emerges from the back of the grid to score his first Formula E points
January 19, 2026
Expo AV expands Martin Audio fleet
January 19, 2026