Qaasid News
Download Our App
Latest News from Pakistan
Junaid Safdar’s colourful mehndi celebration held in Lahore
January 16, 2026
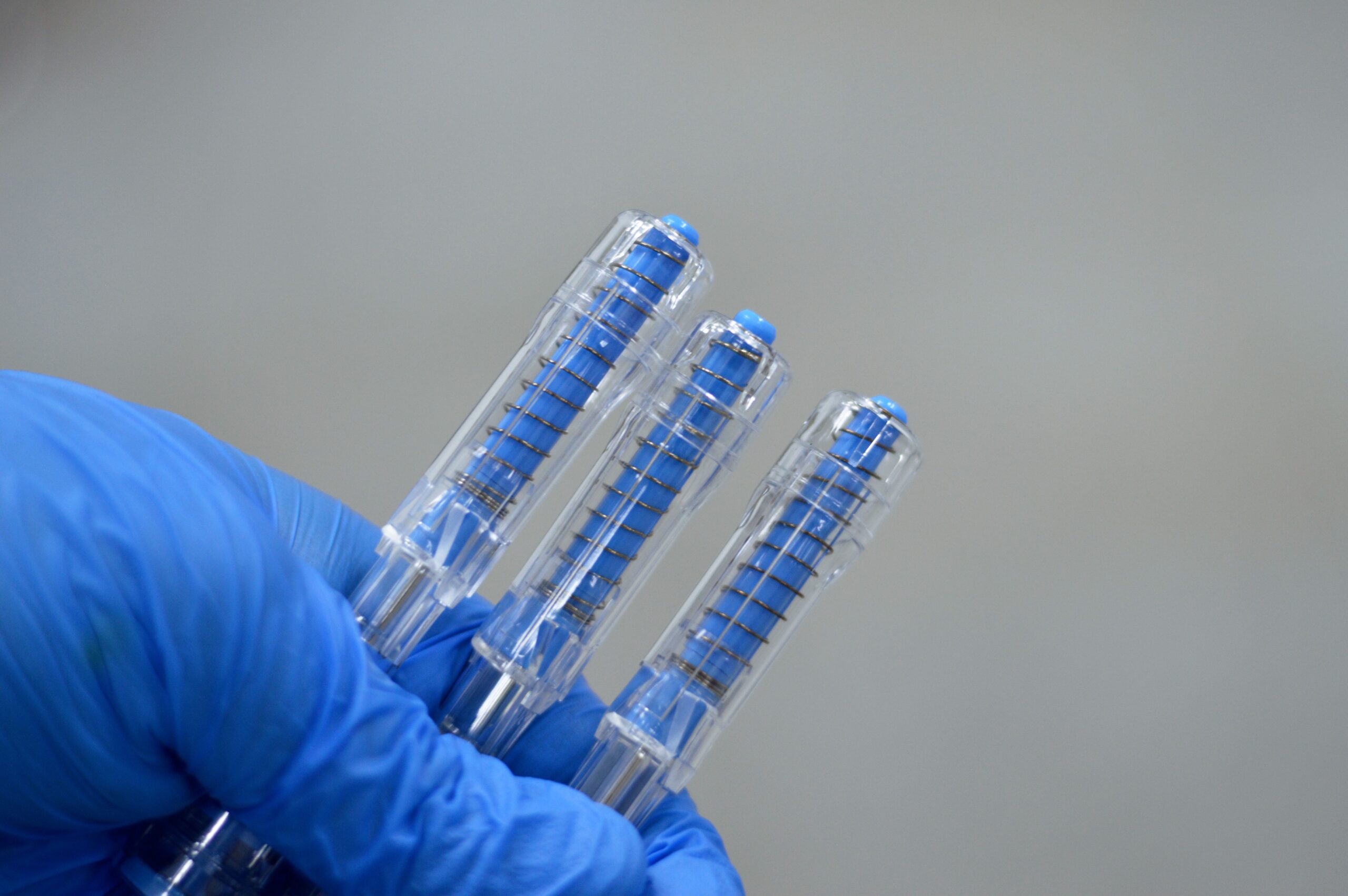
France Expands BOT–BAL Immunotherapy Access for Ovarian Cancer and Soft Tissue Sarcoma
January 16, 2026
6 Best Massage Guns for Quick-Fire Workout Recovery in 2026
January 16, 2026
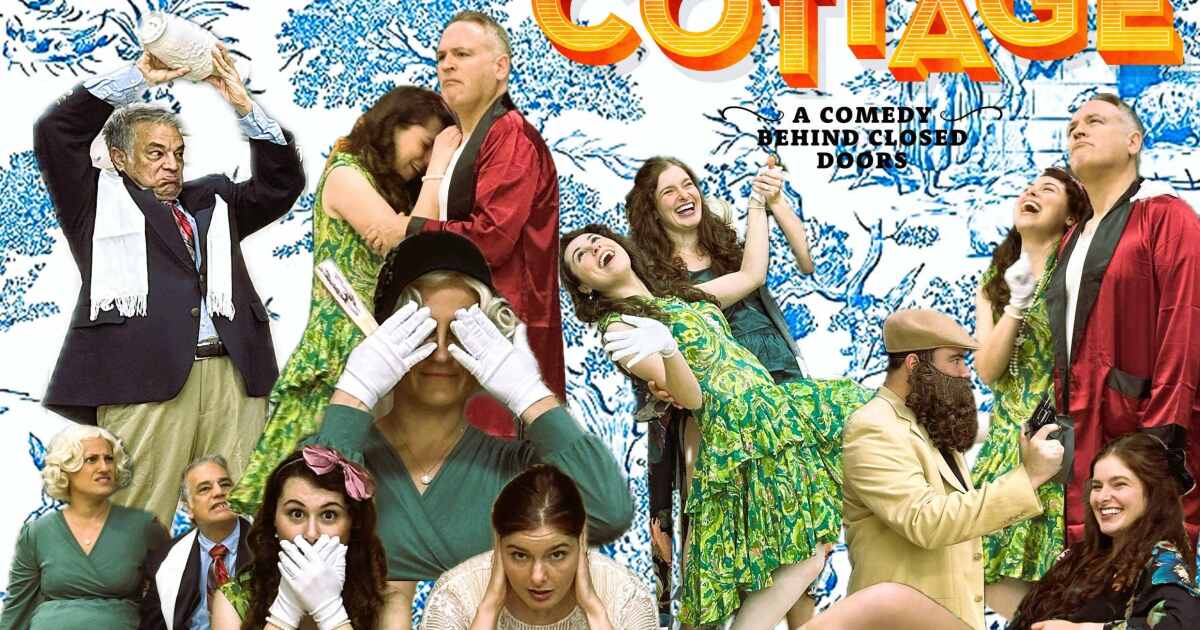
Studio Players’ ‘The Cottage’ a farce written by the playwright who created the stage play ‘Clue’
January 16, 2026
30-Day High-Fiber Meal Plan to Help Lower Cholesterol
January 16, 2026
2026 All-Star starters to be announced Monday on NBC/Peacock at 2 p.m. ET
January 16, 2026
7 K-Beauty Trends Shaping 2026
January 16, 2026
European regulator warns airlines not to fly in Iranian airspace – Reuters
January 16, 2026
Coming Soon With Benefits For Millions Of Phones
January 16, 2026
US floats expanding Gaza ‘Board of Peace’ to other global hotspots
January 16, 2026