Qaasid News
Download Our App
Latest News from Pakistan
Pause on Immigrant Visa Issuances for Pakistani Citizens
January 16, 2026
President, PM felicitate Muslims on Shab-e-Meraj – RADIO PAKISTAN
January 16, 2026
COVID-19 Booster Messaging in Emergency Departments Shows Limited Impact
January 16, 2026
Ant and Dec launch their first podcast, Hanging Out, as part of new Belta Box platform
January 16, 2026
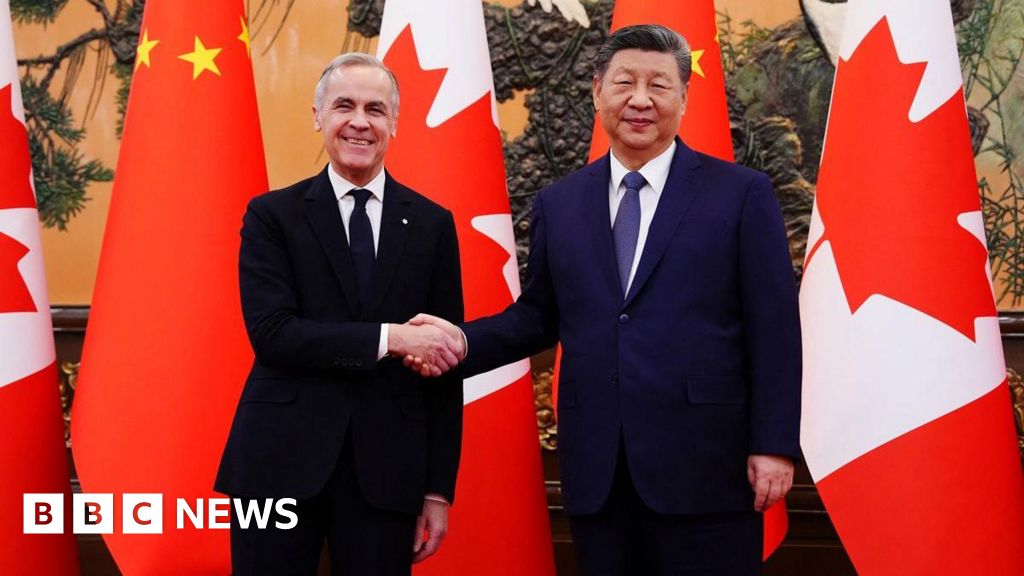
China and Canada announce tariffs relief after a high-stakes meeting
January 16, 2026
NASA Executes Rare Medical Evacuation From the International Space Station – SciTechDaily
January 16, 2026
Israel sees spike in PTSD and suicide among troops as Gaza war persists
January 16, 2026
Shehbaz Sharif launches health card scheme – RADIO PAKISTAN
January 16, 2026
Free Lego deal: Lego is giving away exclusive Burger Bike Carts for free on Jan. 18
January 16, 2026
PTA blocks over 1.4 million links as courts step in over judge smear campaigns
January 16, 2026