Qaasid News
Download Our App
Latest News from Pakistan
BIS statement of commitment to the FX Global Code
January 15, 2026
Shinyakozuka Men’s Fall 2026 Ready to Wear Runway, Fashion Show & Collection Review
January 15, 2026
Forest loss is driving mosquitoes’ thirst for human blood
January 15, 2026
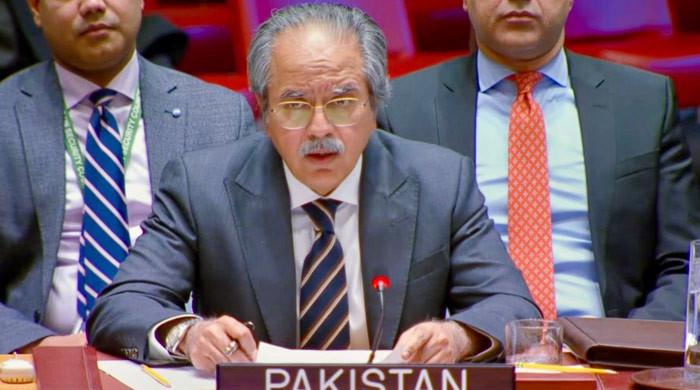
At UNSC, Pakistan urges inclusive talks to end Yemen conflict
January 15, 2026
Hed Mayner Men's Fall 2026 Ready-to-Wear Collection [PHOTOS] – WWD
January 15, 2026
NEOC issues weather alert regarding cold wave expected in different parts of country – RADIO PAKISTAN
January 15, 2026
Ross County condemns ‘small number of young fans’ after flare thrown
January 15, 2026
Iran Closes Tehran Airspace to Flights as Tensions With US Mount – Bloomberg.com
January 15, 2026
Social media users urged to remove ‘illegal, hateful’ content immediately
January 15, 2026
Aseefa highlights strong potential for enhanced cooperation b/w Pakistan, Bahrain – RADIO PAKISTAN
January 15, 2026



![Hed Mayner Men's Fall 2026 Ready-to-Wear Collection [PHOTOS] – WWD](https://afnnews.qaasid.com/wp-content/uploads/2026/01/Hed_Mayner_br____Fashion_Show___02.jpg)

