Qaasid News
Download Our App
Latest News from Pakistan
Polyamines reshape protein phosphorylation to guide key cellular fate decisions
January 15, 2026
Iran protests LIVE: India plans evacuation of nationals from Iran, official sources say
January 15, 2026
Several nations eying JF-17 jets, says PM – Dawn
January 15, 2026
Apple Unveils Apple Creator Studio, Apple’s Bet, Potential Risk Factors
January 15, 2026
Aurangzeb urges MNCs to update business models – Dawn
January 15, 2026
Can Pakistan afford regime change in Iran?
January 15, 2026
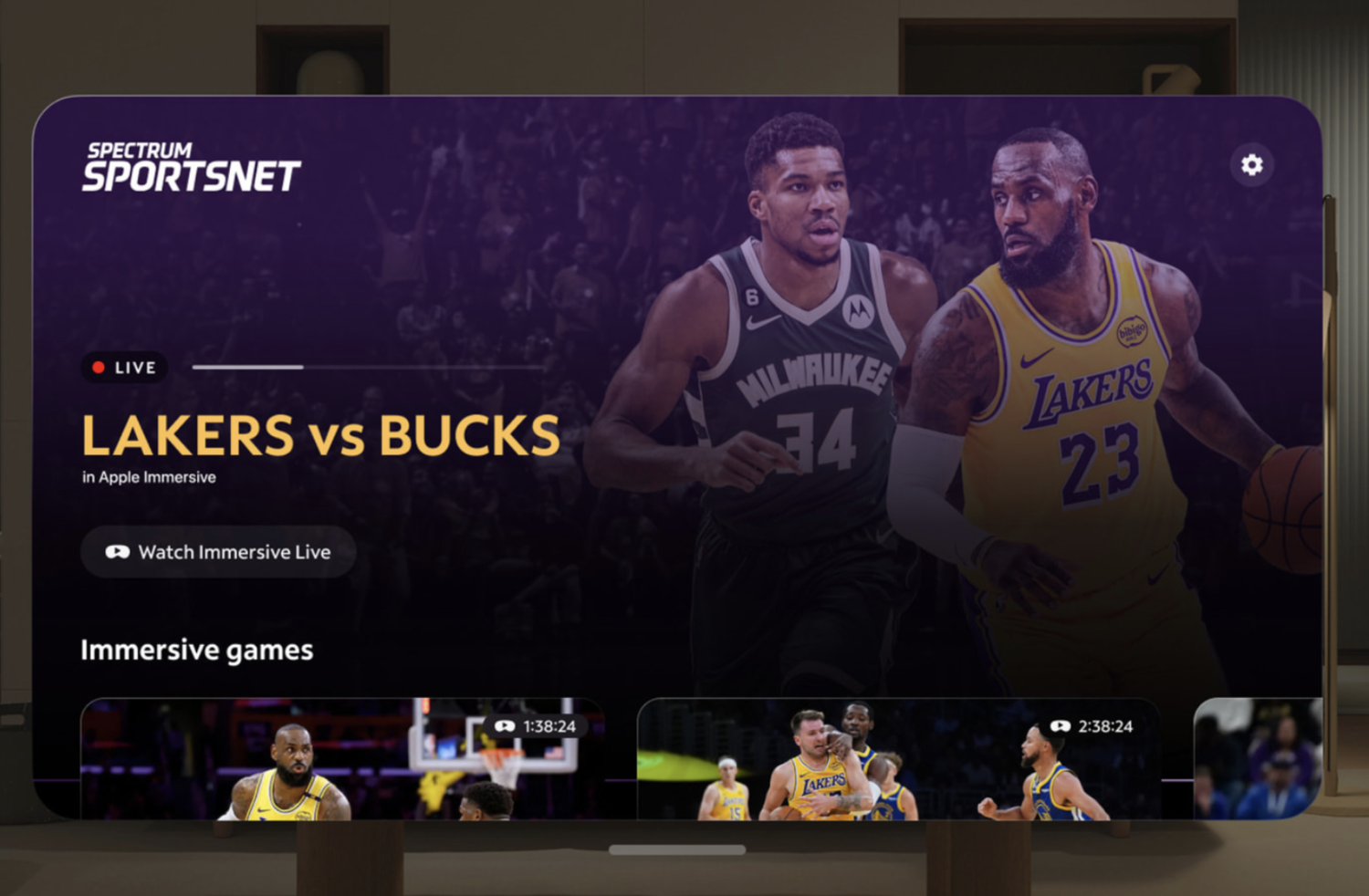
My Impressions Watching LA Lakers in Apple Immersive Video
January 15, 2026
New Insights Into Cell Protein Cleanup System
January 15, 2026
5 Chloé Zhao Movies Ranked By Tomatometer (Hamnet)
January 15, 2026
Signs point to ‘imminent’ US attack on Iran – Dawn
January 15, 2026