Qaasid News
Download Our App
Latest News from Pakistan
What karaoke taught Elizabeth McCracken about fiction— Harvard Gazette
January 13, 2026
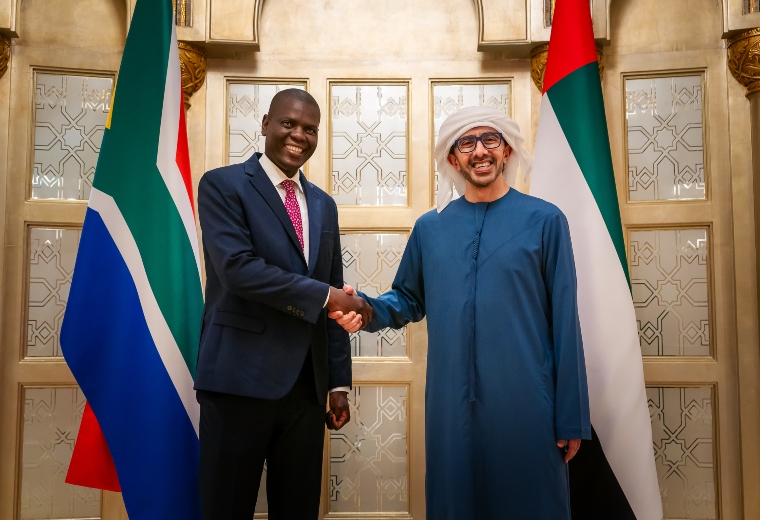
Abdullah bin Zayed, South African Minister of International Relations & Cooperation discuss enhancing ties
January 13, 2026
Statement by Taoiseach Micheál Martin on the passing of Seán Ó Sé
January 13, 2026
USU Production of ‘Natasha, Pierre & the Great Comet of 1812’ Earns Accolades
January 13, 2026
From campus to Milano-Cortina: The NCAA roots behind Team USA women’s hockey
January 13, 2026
Karachi cold wave eases as temperatures slowly rise
January 13, 2026
Rediscover your playful past with Nintendo Switch 2025 Year in Review
January 13, 2026
Powell named Assistant Athletic Director for Compliance
January 13, 2026
New, Sustainably Built Lakewood Medical Offices To Open
January 13, 2026
Abdullah bin Zayed meets Uzbek Deputy PM on sidelines of Abu Dhabi Sustainability Week
January 13, 2026