Qaasid News
Download Our App
Latest News from Pakistan
Why Arab states are silent about Iran’s unrest – The Economist
January 13, 2026
Orlando Magic 5K (Downtown) – City of Orlando
January 13, 2026
As Iran faces unrest, Israel waits quietly for Trump’s next move
January 13, 2026
Taliah Lee Notched Defensive Player of the Week and Moved Up in the MACU Record Book
January 13, 2026
NASA unveils Artemis 2 launch windows: What we know – Astronomy Magazine
January 13, 2026
Webcast: Consumer Protection Enforcement: DOJ, FTC, and State AGs at the Crossroads
January 13, 2026
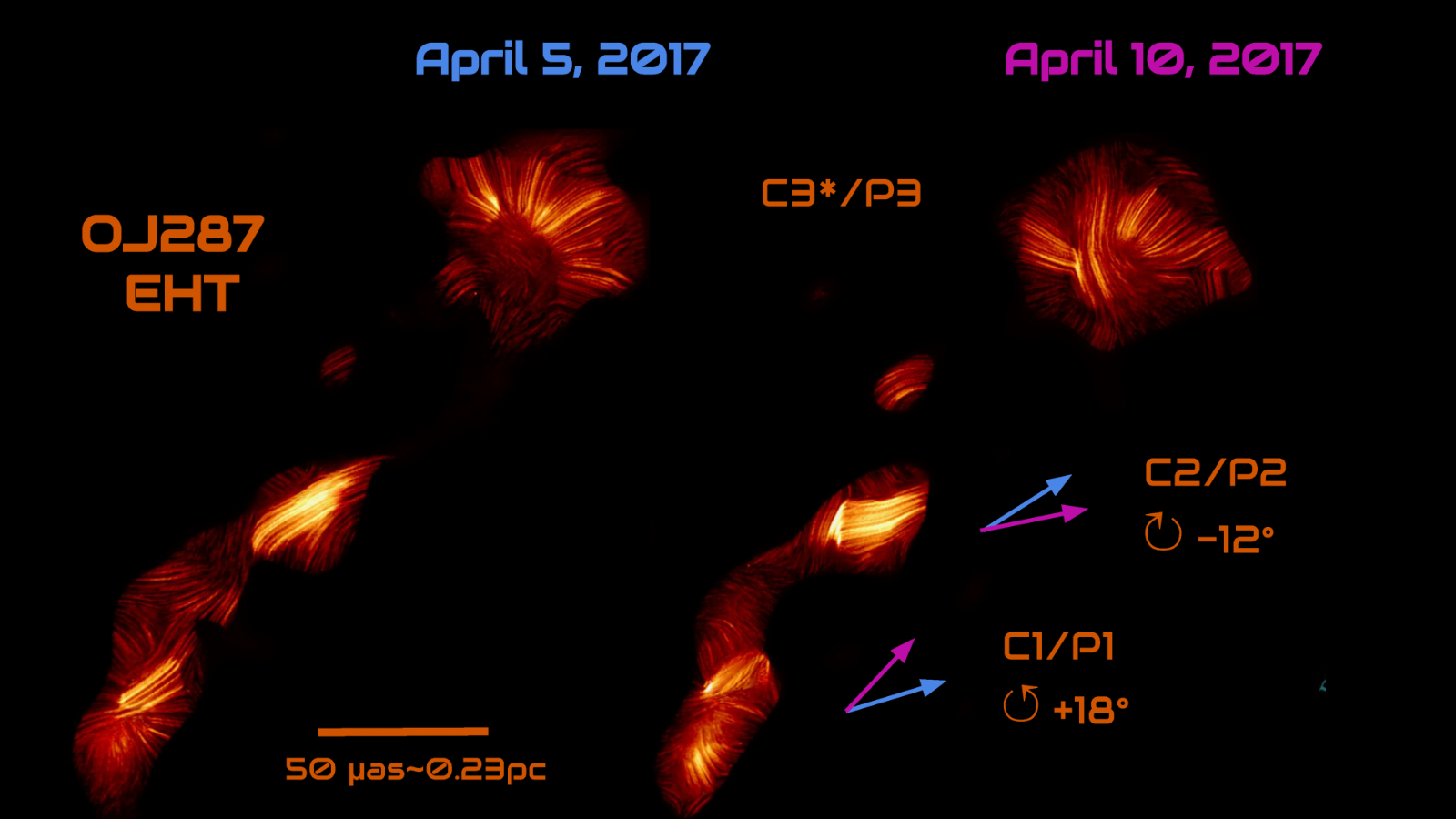
Astronomers watch 2 supermassive black holes caught in a twisted dance with never-before-seen jet behavior
January 13, 2026
Taking a fresh look at definition of autism — Harvard Gazette
January 13, 2026
New JBL Endurance Zone open earbuds: where to buy
January 13, 2026
President arrives in Manama on four-day official visit to Bahrain – RADIO PAKISTAN
January 13, 2026