Study design and setting
This was a facility-based cross-sectional study conducted from September to October 2021. Participants were enrolled at ANC contact in the public health facilities providing comprehensive emergency obstetric and newborn care in three regions of Unguja Island (Mnazi Mmoja Hospital from the Urban-west region, Kivunge Hospital from the North A region, and Makunduchi Hospital from the southern region). Unguja regions are composed of two districts each, and from each region, one district was selected purposively according to the population covered. The urban region has a total population of 593,678, of which 370,645 are in the Urban-West district. The North region has a total population of 187,455, of which 105,780 are from the North A district. The southern region has a total population of 115,588, of which 76,346 are from the Central-south district (Ministry of Finance, 2013). In Zanzibar, the Focused Antenatal Care (FANC) guideline recommends that all pregnant mothers to attend four or more ANC visits to monitor the pregnancy for timely identification of pregnancy complications and risk factors and early management; the first antenatal contact should take place before 16 weeks of pregnancy for early detection and management of problems. Despite the high coverage of the first ANC contact of 91.1%, only 31.3% of women had completed four or more ANC contacts in Zanzibar [32].
Study participants
Pregnant women who were followed up after ANC contact and who voluntarily consented to participate in the study were included in the study in selected public health facilities of Unguja. The target population was all pregnant women attending ANC in selected public health facilities of Unguja during the study period.
Sample size
The required sample size was determined by using a single population proportion formula.
$$mathrm n=frac{;mathrm Z^2;mathrm x;mathrm p;(100;-mathrm p)}{mathrm E^2}$$
Where n is the minimum sample size, Z is the Z value (1.96 for a 95% confidence interval), E is the minimum acceptable error, which is 5% (0.05), and p is the proportion or prevalence that meets our criteria. The proportion was taken from the study done in Nigeria, with a prevalence of 36% of pregnant women satisfied with the antenatal care services at the health facility.
Therefore:
$$mathrm n=frac{1.962;times:0.36;(100-0.36)}{5^2}$$
The required sample size is therefore 354.
The researcher assumed that there was a non-response to the study, which was estimated by calculating the adjusted factor.
$$mathrm{Adjusted};mathrm{factor};=;mathrm n;(100/100-mathrm f;%)$$
where n is the required sample size and f is the non-response rate.
The non-response rate is therefore 10%.
Given these values, the minimum sample size was arrived at thus:
$$mathrm N=;frac{mathrm n;times;(100);}{100%-10%}$$
That is,
$$mathrm N;=;frac{354;times;(100);}{100%-10%};;$$
Therefore, the minimum sample size = 393
Sampling technique and determining the number of study participants per health facility
Purposive sampling was used to select the region, district, and health facilities. Three public facilities were selected intentionally as they captured large populations and were the only public health facilities that provided Comprehensive Emergency Obstetric and Newborn Care (CEmONC) in Unguja.
Systematic random sampling was used to select study participants from the three selected hospitals. The number of pregnant women recruited from each hospital was determined by calculating the percentage required for each facility, the average number of pregnant women booking for ANC per month at Mnazi Mmoja Hospital (numerator value) 300, Kivunge Hospital 80 and Makunduchi Hospital 70, this fraction (numerator/denominator) is then multiplied by the hundred per cent to determine the percentage of pregnant women to be recruited from each Health facility.
|
Pregnant women booking for ANC per month at Mnazi Mmoja Hospital |
||
|
Therefore, (frac{300;times;100}{450}=;67%) |
(frac{67;mathrm x;393}{100}=;263) |
|
|
Pregnant women booking for ANC per month at Kivunge Hospital |
||
|
Therefore, (frac{80times100;=;17%}{;450}=;17%) |
(frac{17times393;}{100}=;67) |
|
|
Pregnant women booking for ANC per month at Makunduchi Hospital |
||
|
Therefore, (frac{70times100}{450};=;16%) |
(frac{16times393}{100}=;63) |
|
Thus, 263 pregnant women were recruited from Mnazi Mmoja Hospital, 67 from Kivunge Hospital, and 63 from Makunduchi Hospital.
Variables and measurement
The quality of antenatal care was calculated at the facility level, while client satisfaction was determined at the individual level. We used a questionnaire that contained socio-demographic characteristics, the obstetric profile of pregnant women, and characteristics of the health facilities to measure pregnant women’s level of satisfaction, and factors associated with quality antenatal care services.
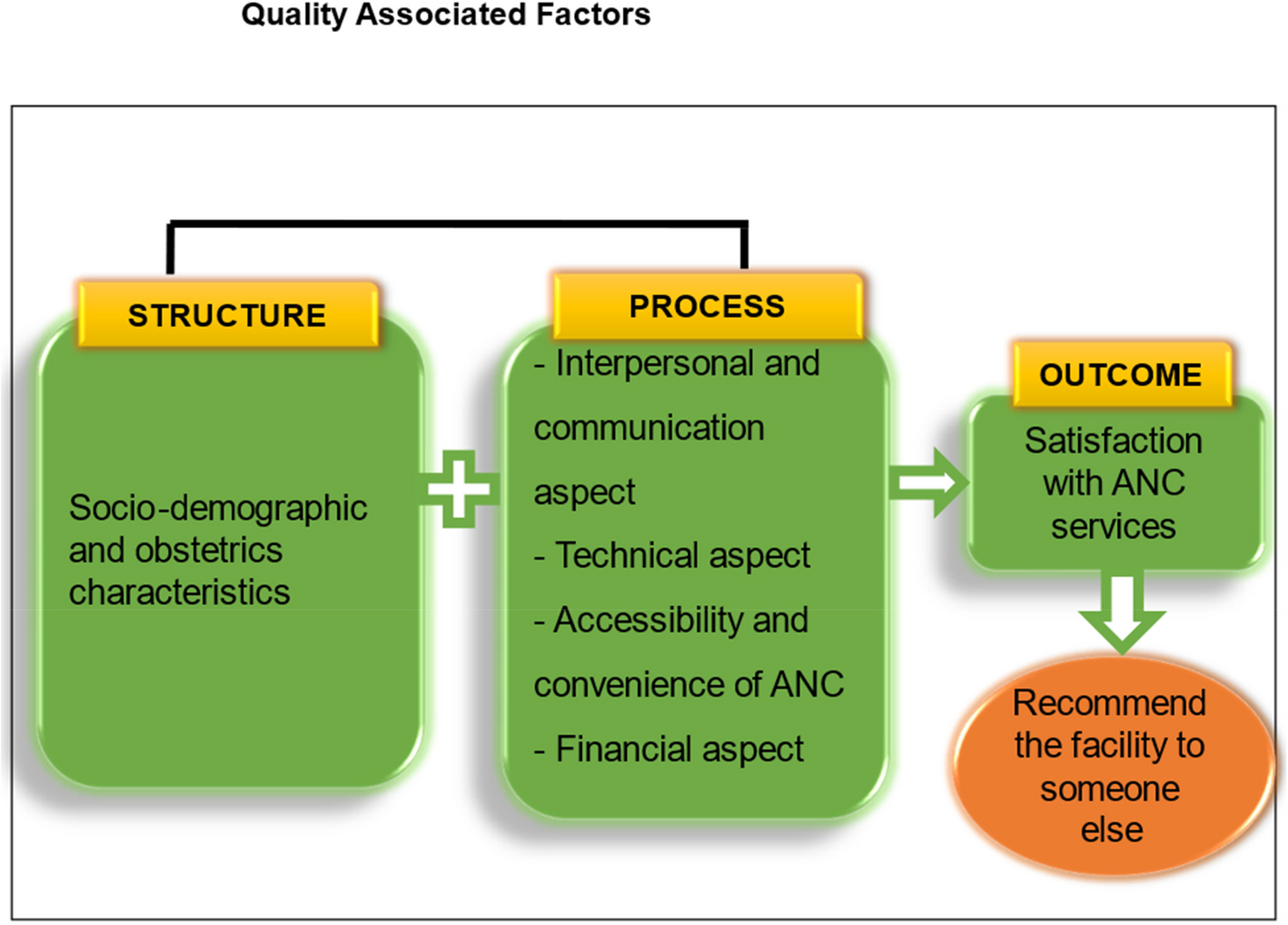
The outcome variable was ANC client satisfaction computed by combining women’s responses to a series of questions regarding the ANC contact using a long-form Patient Satisfaction Questionnaire (PSQIII) [3, 24, 33]. This Likert scale questionnaire proposed five dimensions of patient satisfaction with ANC services. These were interpersonal and communication aspects, technical quality aspects, financial aspects, accessibility and convenience, and general satisfaction with ANC services. Each domain was tested through different related questions, which was vital in identifying a particular area to improve the quality of maternal and neonatal care services. General satisfaction with ANC services provided to pregnant women in health facilities was determined by using a 5-point scale in descending order: very satisfied (5 points), satisfied (4 points), neutral (3 points), unsatisfied (2 points), and very unsatisfied (1 point). Finally, the overall satisfaction index was developed by categorizing the sum of scores into a three-point Likert scale, very satisfied as high satisfaction, and satisfied as moderate satisfaction. Neutral, unsatisfied, and very unsatisfied were merged as low satisfaction. Neutral responses were classified as unsatisfied, considering that participants may be fearful of expressing dissatisfaction.
Finally, the overall satisfaction was measured using the following operational definitions: high satisfaction with ANC services (coded 3) is when a pregnant woman scored 22 to 35 of the satisfaction measurement items; moderate satisfaction (coded 2) is when a pregnant woman scored 15 to 21; and low satisfaction (coded 1) is when a pregnant woman scored ≤ 14.
Data collection
Data collection methods
Face-to-face interviews using structured questions were used to collect information about socio-demographic and obstetric characteristics, general satisfaction, technical quality, interpersonal and communication aspects, financial aspects, and accessibility and convenience of the ANC services. A pre-programmed smartphone-based application, Kobo tool kit, was used. The data were then transferred to the computer for analysis, and SPSS version 26 was used to analyze the data. The data collection form was exported to the tablets to be used for analysis. The principal investigator, together with two female nursing officers who assisted with the data collection procedure during the ANC contact, conducted exit interviews with pregnant women.
Data collection instruments
A questionnaire exported to tablets was used to obtain information about patient satisfaction. The PSQIII was exported to tablets for data collection. It has been validated for use in different settings [24, 33] and was modified to be used in this study. The questionnaire consists of 75 items that measure the level of satisfaction with quality ANC services, that is, interpersonal and communication aspects, technical quality aspects, financial aspects, accessibility and convenience, and general satisfaction with the ANC services. The modified questionnaire was first developed in English and then translated into the local language (Kiswahili) and back-translated to English by the language professional editor for clarity.
Operational definitions
The ANC was defined as health care given to a woman during pregnancy, while the waiting time in this study was defined as time spent from the end of the health talk to the beginning of the clinic consultation.
Data quality control
To ensure the quality of data management, the adapted questionnaire was prepared in English and translated into the local language. Three days of training were performed/conducted for two female data collectors (nurse officers), and there was close supervision by the principal investigator during the pretest of the tool and the data collection procedures. The questionnaire was pre-tested in a hospital, which was not selected for inclusion in the study. After the essential modifications and corrections of the questionnaire had been validated, the reliability (internal consistency of the instrument) was checked by Cronbach’s alpha. All domains that had a Cronbach’s alpha of 0.70 or higher are considered acceptable. The principal investigator checked the data every day for completeness and consistency before uploading it to the computer for analysis. Data collectors were required to correct any missing values and resolve inconsistencies before leaving the field after collecting the data.
Data processing and analysis
Statistical analysis was performed to analyze the data. SPSS software (version 26.0) was used for descriptive and logistic regression analyses. Categorical data were summarized using frequency and percentages, while continuous variables were summarized using mean and standard deviation. In logistic regression, both binary and multivariable analyses were carried out to determine factors that influenced the level of satisfaction, that is, high, moderate, or low levels of satisfaction. The p-value of 0.05 or less was considered statistically significant, and adjusted odds ratios were found to assess the strength of the association between variables.