The patient, female, Ms. Yang, 39 years old, had a history of good health. She had two full-term vaginal deliveries and two induced abortions. Her menstruation was regular, and her last menstrual period was on April 16, 2024. Her antenatal examinations were irregular. The blood glucose level was 12.0 mmol/L one hour after the oral glucose tolerance test. At 34+3 weeks of pregnancy, her blood pressure (BP) was 136/81 mmHg, and the urine protein was ±. On December 27, 2024, at 36+3 weeks of pregnancy, she occasionally had lower abdominal pain in the morning. At 17:26, the abdominal pain worsened. She took a private car to the hospital and gave birth to a baby boy in the private car at about 18:00. The placenta had been delivered. She arrived at the emergency department of Affiliated Hospital of Jining Medical University at 19:06, and her blood pressure was 134/75 mmHg. After admission, the uterine contractions were poor, and oxytocin was given to enhance the uterine contractions. At 19:44, the blood pressure was measured at 165/99 mmHg, and 10 mg of nifedipine was given orally. At 20:14, the blood pressure was 155/100 mmHg, and at 20:30, the blood pressure was 185/108 mmHg. 20 mg of nifedipine was given orally, and magnesium sulfate was infused by pump. At 21:00, eclampsia suddenly occurred. Rescue measures were taken (opening the airway, using a tongue depressor to prevent tongue bite, turning the head to one side, oxygen inhalation, intravenous injection + pump infusion of magnesium sulfate, and intravenous infusion of mannitol). After that, the eclampsia was controlled. At 21:30, the blood pressure was 123/78 mmHg, and the patient could be awakened and did not complain of any discomfort. An urgent examination showed that the hemoglobin was 116 g/L, the platelet was 82 × 10⁹/L, and the urine protein was 3+. At 22:00, the patient developed nausea, vomiting, and right upper abdominal pain. At 22:30, the blood pressure suddenly dropped to 82/51 mmHg, the pulse rate (P) was 82 beats per minute, the respiratory rate (R) was 20 breaths per minute, and the oxygen saturation was 99%. The blood pressure decreased progressively, reaching a minimum of 66/37 mmHg, and the pulse rate was 83 beats per minute. After the anesthesiologist arrived, norepinephrine and adrenaline injection were given to raise the blood pressure. An urgent blood gas analysis showed that the hemoglobin was 66 g/L. Considering the patient’s postpartum eclampsia, the possibility of the HELLP syndrome and subcapsular hepatic hematoma could not be excluded. Rapid fluid replacement was given, and 10% calcium gluconate was added to the infusion for intravenous drip. A bedside color Doppler ultrasound examination was arranged. The B-ultrasound showed a large amount of abdominal effusion. Under the guidance of the ultrasound, abdominal paracentesis was performed, and non-clotting blood was drawn out. There was a high suspicion of the HELLP syndrome and rupture and bleeding of the subcapsular hepatic hematoma, and exploratory laparotomy was carried out. During the operation, a large amount of bright red non-clotting blood, about 3000 ml, was found in the abdominal cavity. The hepatic capsule on the diaphragmatic surface of the right lobe of the liver was widely peeled off, with obvious oozing of blood. The hepatoduodenal ligament was edematous, and the liver showed severe fatty liver changes. An attempt was made to compress the bleeding site with a gauze pad, but the effect was not good. Ligation of the right hepatic artery and the middle hepatic artery + cholecystectomy were performed. After applying hemostatic fibrils on the diaphragmatic surface of the right liver, two and a half pieces of uterine gauze strips were packed in, and a 3-cm incision was made on the right abdominal wall to lead out and fix them. One abdominal drainage tube was placed under the right liver, above the left liver, and in the pelvic cavity respectively and fixed. The estimated blood loss during the operation was about 8000 ml. During the operation, 22 units of leukocyte-reduced suspended red blood cells, 2200 ml of plasma, 10 units of cryoprecipitate, 2 therapeutic doses of platelets, and 7000 ml of infusion were given, and the urine output was about 50 ml. After the operation, the patient was transferred to the intensive care unit.
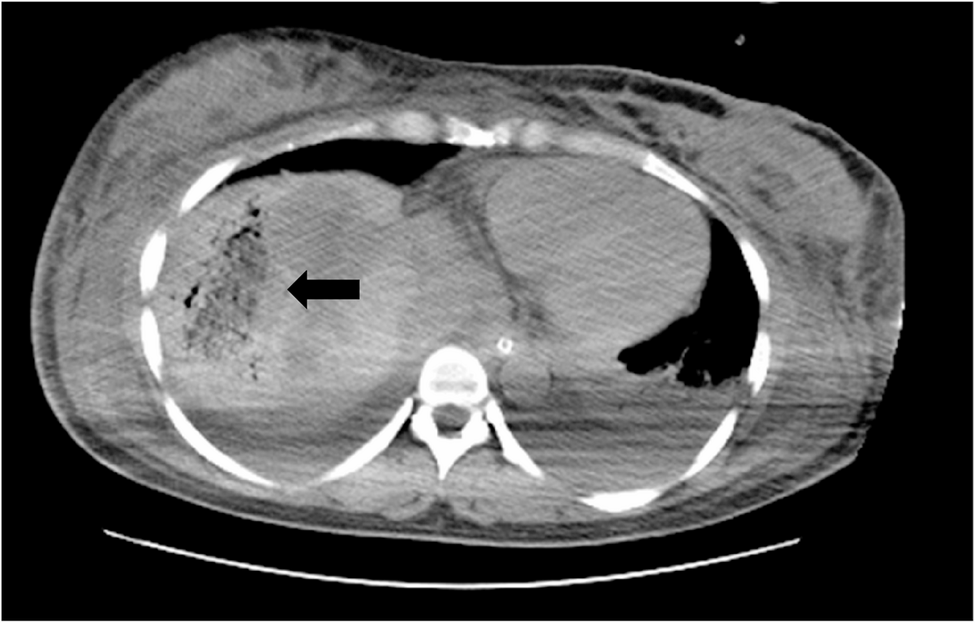
After the operation, a large amount of vasopressor drugs were needed to maintain the blood pressure. The drainage volume of the three drainage bags was 1000 ml within less than 1 h. There was extensive bleeding from the surgical wound, severe shock, (disseminated intravascular coagulation) DIC, and abnormal coagulation. The drawn blood did not coagulate. The blood gas analysis showed that the lactate was greater than 10 mmol/L several times, and the highest was greater than 20 mmol/L. A multidisciplinary discussion involving departments such as Hepatobiliary Surgery, Gastrointestinal Surgery, Intensive Care Unit, Cardiology, Blood Transfusion Department, and Hematology Department was conducted across the hospital. To maintain blood pressure, a large dose of norepinephrine (186 mg in total within 24 h after surgery) was infused via pump, combined with 24 units of pituitrin and 0.5 mg of epinephrine. The ventilator was used to assist breathing, and organ function support treatment and blood transfusion were given. On the second day after the operation, the vasopressor drugs were stopped, and blood transfusion was continued. The patient was in anuria, with renal failure and obvious general edema, and plasma exchange was given. Fragmented red blood cells were found in the peripheral blood smear, suggesting hemolysis, which further confirmed the HELLP syndrome. The biochemical indexes deteriorated rapidly after the operation. On December 29, the alanine aminotransferase (ALT) was 3629.3 U/L, and the aspartate aminotransferase (AST) was 5034.5 U/L. On December 30, the lactate dehydrogenase (LDH) was 3993.7 U/L. The patient’s coagulation function improved, but there was persistent thrombocytopenia. A large amount of accumulated blood around the liver was found on the CT scan (Fig. 1).From January 1 to January 6, 2025, the platelet count fluctuated between (3–9)×10⁹/L. The provincial medical team was reported. The treatment mainly includes hormones, plasma exchange, and immunoglobulin, etc. Platelet transfusion must be extremely cautious and should be avoided in cases of non-fatal active bleeding to prevent the condition from deteriorating further. Imipenem and cilastatin combined with vancomycin were continued for anti-infection treatment, liver protection, maintaining renal perfusion, continuous renal replacement therapy treatment, continuous plasma exchange, application of intravenous immunoglobulin, and 60–80 mg of methylprednisolone was given once a day. On January 10, 2025, the blood urea nitrogen was 34.86 mmol/L, and the creatinine was 552.8 µmol/L. The CT scan showed a small amount of subarachnoid hemorrhage in the right parietal lobe, and antiepileptic treatment was given. On January 11th, the CT scan showed that the accumulated blood around the liver had decreased (Fig. 2).There was a large amount of pleural effusion accompanied by atelectasis, and thoracentesis and drainage were performed for 24 days. Imipenem + vancomycin was used for treatment for 10 days after the operation, and then it was downgraded to omadacycline + piperacillin/tazobactam for 12 days, and then it was changed to moxifloxacin for 6 days. The patient’s liver and kidney functions and platelet count gradually returned to normal, and the hormones were stopped. A total of 4 multidisciplinary case discussions were organized in the whole hospital, and the provincial treatment expert group and the remote consultation of Ruijin Hospital in Shanghai were invited many times. A total of 52 units of leukocyte-reduced suspended red blood cells, 8250 ml of plasma, 90 units of cryoprecipitate, 11 therapeutic doses of platelets, and 6 plasma exchanges (2500 ml of plasma was used each time) were given. The patient was cured and discharged 40 days after the operation. No abnormalities were found during the one-month follow-up after discharge.(Table 1).
On December 30, 2024, a reticular shadow was visible adjacent to the diaphragmatic top of the right hepatic lobe, with a large amount of hematocele around it, measuring 3.6 cm × 2.0 cm × 2.8 cm
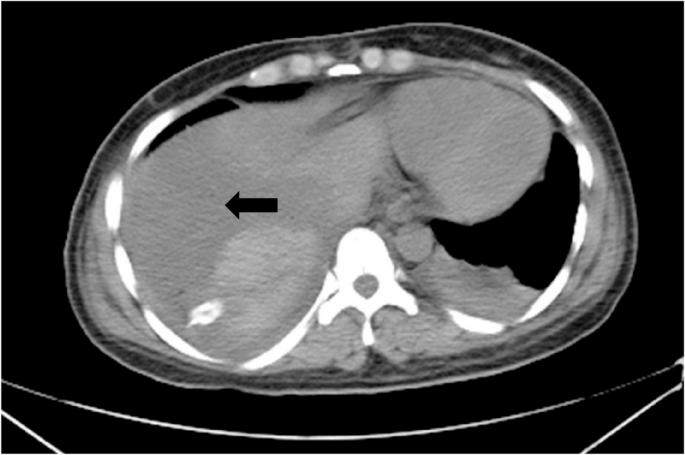
On January 11, 2025, there was still hematocele around the diaphragmatic top of the right hepatic lobe, with the range reduced to approximately 2.5 cm × 1.5 cm × 1.7 cm, the density decreased, and the boundary was clearer than before
Reference values: White blood cells 3.5–9.5 × 10⁹/L, hemoglobin 115–150 g/L, platelets 125–350 × 10⁹/L, fibrinogen 2–4 g/L, prothrombin time 10–14 S, alanine aminotransferase (ALT) 0–35U/L, aspartate aminotransferase (AST) 14–36U/L, lactic acid 0.5–1.8mmol/l, lactate dehydrogenase 120–250U/L, creatinine 41–73umol/l, urea 2.6–7.5mmol/l, blood pH 7.35–7.45.