For millions of people across the UK, migraine is a debilitating disease. There is clear evidence that patients struggle to receive a timely diagnosis and access to effective treatments varies across the UK. Upskilling pharmacy teams, particularly in community and primary care, could help improve support for patients.
This was the overarching message from a roundtable meeting, hosted by The Pharmaceutical Journal at the Royal Pharmaceutical Society (RPS) London headquarters on 1 July 2025.
The roundtable sought to explore the current state of practice in the UK and discuss how the role of pharmacy could be optimised to provide more effective pharmaceutical care for patients with migraine. It incorporated findings from a survey of 304 pharmacists across community, primary care and hospital sectors undertaken by The PJ between 20 May and 11 June 2025.
The event brought together a range of migraine experts from across the UK, including pharmacists, members of the wider multidisciplinary team and the charity sector (see ‘Panel members’, below) and was co-chaired by Alex Clabburn, senior editor, and Caitlin Killen, clinical editor, at The PJ.
More than half of people with migraine lack adequate support
Migraine is the second biggest cause of disability worldwide and affects up to 10 million people in the UK.
Despite this, “too many people don’t understand it”, said Rob Music, chief executive of the Migraine Trust.
Contrary to popular belief, migraine is “not just a pain” but affects all areas of a person’s life, he added.
According to a 2024 survey of 2,208 people living with migraine, conducted by the Migraine Trust, 60% said their work or study was “very much affected” by migraine; 80% said their condition had caused them to participate less in social activities; 89% said their mental health had been affected; and 39% had had thoughts of suicide because of their condition.
It is concerning that 63% disagreed or strongly disagreed that they felt supported by the healthcare system, with Music adding that patients with migraine often feel ignored and frustrated.
He also highlighted a “lack of equity around care for migraine” that included variation across the UK and 41% of people from a Black, Asian or minority ethnic background needing to see a healthcare professional five or more times before diagnosis.
Migraine and headache account for 2.5 million primary care appointments each year, and patients are increasingly seeking support directly from emergency care, with A&E attendance for migraine rising by 22% in 2023/2024, Music shared.
According to NHS England, an estimated 16,500 emergency admissions for headaches and migraine attacks could be avoided with the right treatment pathways in place, while nearly £1m a year could be restored to the UK economy through improved productivity, with just a 10% improvement in migraine care.
Music told the roundtable that current National Institute for Health and Care Excellence (NICE) treatment pathways are “terrifyingly out of date” [NB: see Box], meaning that pharmacists, GPs and other clinicians struggle to advise patients with confidence, while pressures on the healthcare system and difficulties with accessing GP appointments also present barriers to diagnosis.
Box: NICE guidance
Prior to The PJ survey on migraine being sent out and the roundtable meeting, calcitonin gene-related peptide inhibitors (CGRPs) were not included in National Institute for Health and Care Excellence (NICE) guideline on ‘Headaches in over 12s: diagnosis and management’.
However, following a surveillance consultation that concluded on 8 May 2025, links to technology appraisal guidance on available CGRPs have now been included.
Pharmacists and pharmacy teams, particularly in community and GP pharmacy, “are really well positioned” to support a new, improved pathway for migraine care, Music said. The PJ survey results suggest a general willingness from pharmacist respondents to take on an enhanced role in migraine care. However, responses also indicate that improvement is needed in the understanding of diagnosis and treatment of migraine, as well as headache more generally.
Paul Stuart
Lack of awareness from patients and clinicians leads to delayed diagnosis
The roundtable highlighted barriers to diagnosis of migraine, beginning with a lack of awareness among both patients and clinicians.
“They think headache is something everybody gets,” said Katy Munro, a senior GP headache specialist at the National Migraine Centre and secretary of the British Association for the Study of Headache. She suggested that migraine can be mistaken for other conditions, such as sinusitis. Clinicians often “don’t want to commit” to a diagnosis of migraine, Munro added.
Other attendees noted that migraine attendance at healthcare appointments, A&E and specialist referrals is often recorded as “pain” or “headache”, making it difficult to follow up.
However, pharmacists in community pharmacy and primary care proved more able to correctly identify migraine symptoms than hospital pharmacists in The PJ survey.
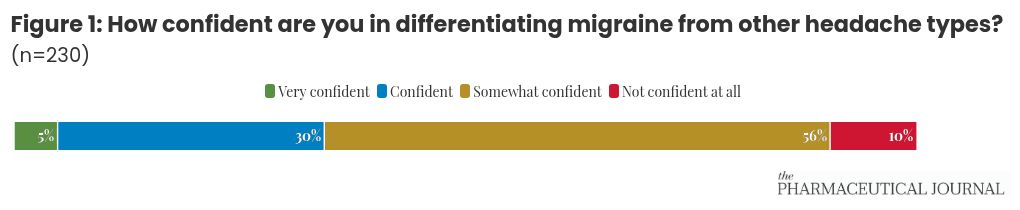
Around 56% of pharmacist respondents (n=129) described themselves as “somewhat confident” about differentiating migraine from other headache types, compared with 34% (n=79) who said they were “confident” or “very confident”.
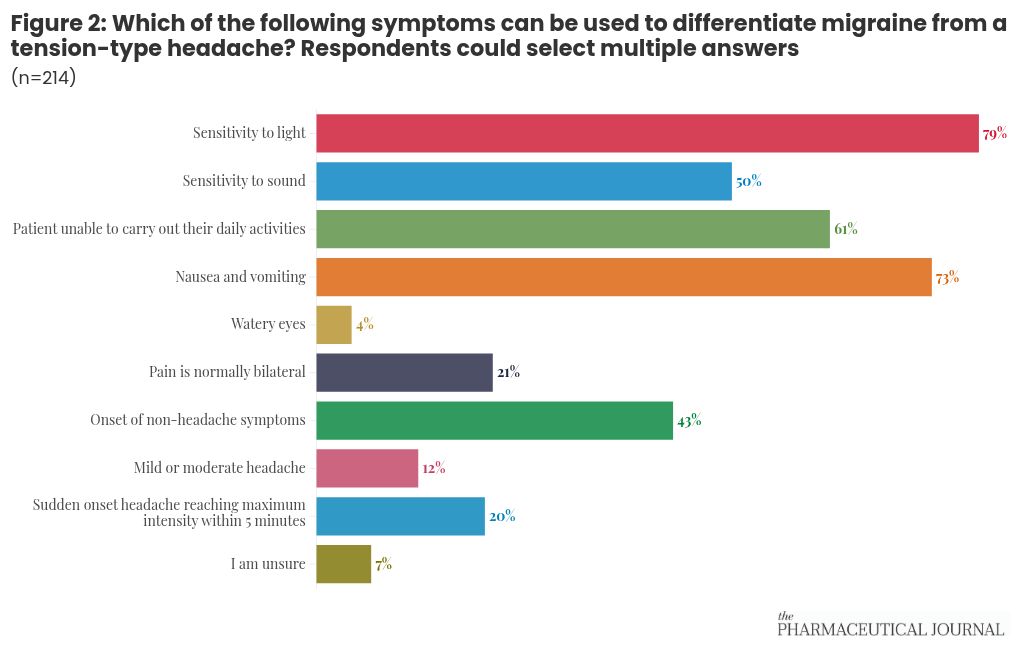
Many pharmacist respondents proved able to identify symptoms that can be used to differentiate migraine from tension-type headache. Eight in ten (79%; n=169) correctly identified sensitivity to light as a migraine differentiator, while 50% (n=106) identified sensitivity to sound and 73% (n=157) selected nausea and vomiting. However, 43% (n=91) incorrectly selected onset of non-headache symptoms, 21% (n=45) responded that migraine pain is normally bilateral and 20% (n=43) selected “sudden onset headache reaching maximum intensity within five minutes”.
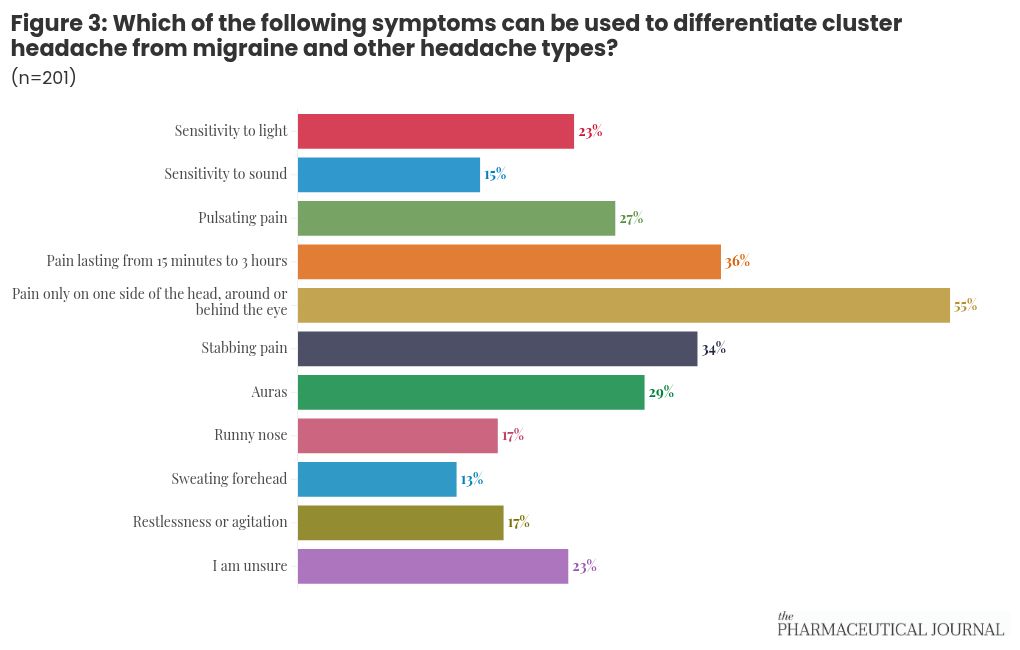
However, pharmacists seem less clear on differentiating cluster headache from migraine and other headache types. More than half (55%; n=111) correctly selected “pain only on one side of the head, around or behind the eye” as a differentiating cluster headache system, while 36% (n=72) selected “pain lasting from 15 minutes to 3 hours” and 34% (n=68) selected “stabbing pain”. Otherwise, the survey found an even spread of incorrect answers and “I am unsure”.
Better training for pharmacy teams could help to identify patients suffering from migraine.
In particular, pharmacy technicians are “quite often with the first pharmacy person [patients] see when they either are in community pharmacy or in hospital”, Diane Torry, editor of The Pharmacy Technician Journal at the Association of Pharmacy Technicians UK, noted.
Pharmacy technicians may therefore be able to notice patterns in patients presenting with symptoms of migraine, a crucial step towards diagnosis.
Optimal treatment pathways and support through pharmacy
Commencing initial treatments
Bethany Hill, a headache and facial pain clinical nurse specialist at Guy’s and St Thomas’ NHS Foundation Trust, highlighted the need for a “layering approach” in treating acute migraine symptoms.
“You have to understand how you use your simple analgesics first. You have to understand how you use your antiemetics first. Then, you have to understand how to use your triptans before you can understand gepants,” she said.
For many patients, over-the-counter remedies and Pharmacy (P) medicines are sufficient to manage migraine symptoms.
Callum Duncan, consultant neurologist at Aberdeen Royal Infirmary, told roundtable attendees that community pharmacy could play a role in “ensuring that acute treatment is done well”.
However, The PJ survey showed mixed levels of awareness of the correct use of analgesics to treat migraine symptoms.
More than half (56%) of pharmacist respondents (n=107) said they were ‘somewhat confident’ in recommending an appropriate treatment for migraine, compared with 34% (n=65) who said they were ‘confident’ or ‘very confident’.
However, 41% of pharmacists (n=77) incorrectly said they would recommend co-codamol to manage migraine symptoms, while nearly 13% (n=24) would also suggest codeine.
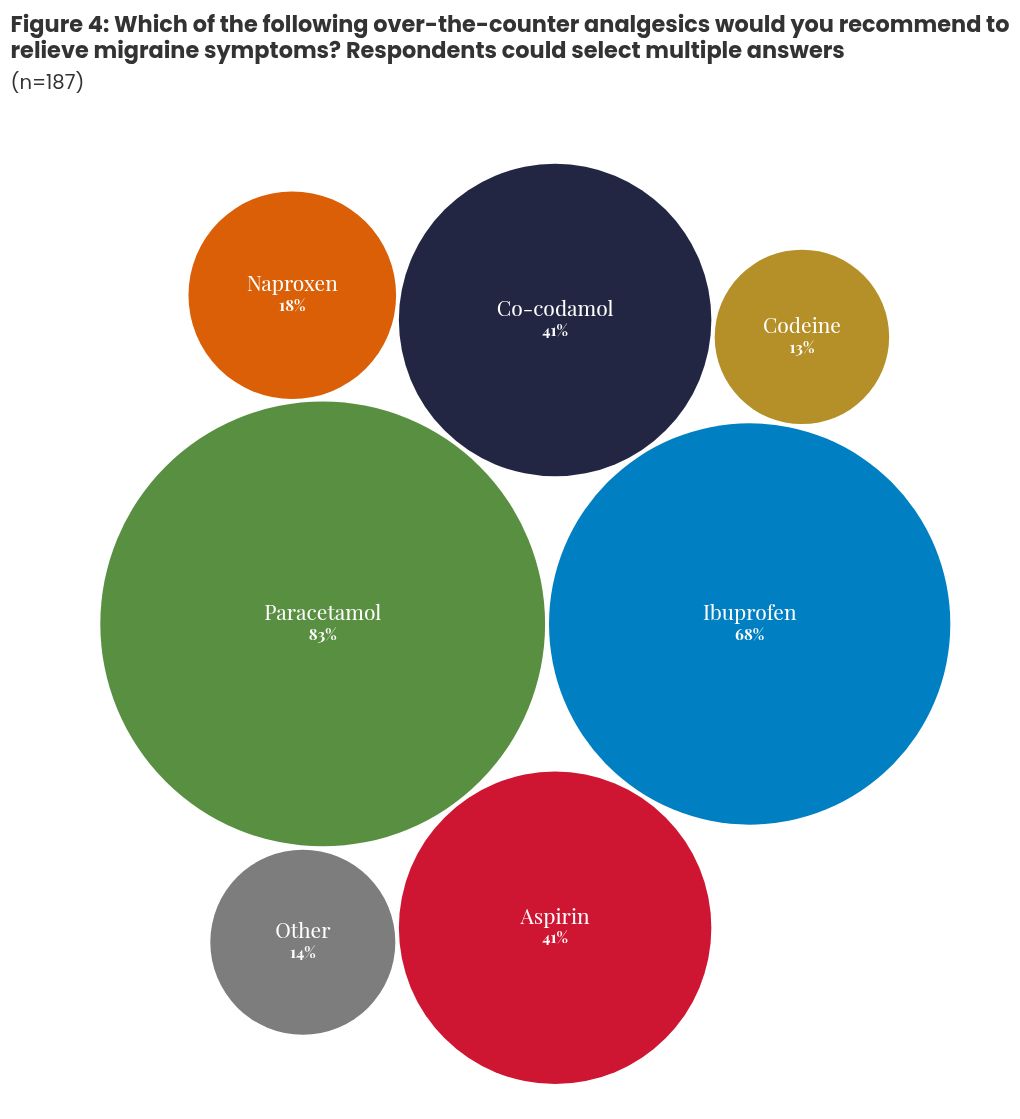
Commenting on the findings, Duncan noted that paracetamol was likely “too weak” to treat migraine, while “aspirin should be standard”.
“Codeine shouldn’t be there at all, co-codamol shouldn’t be there at all,” he said.
If analgesics and anti-emetics prove insufficient, a patient with a previous diagnosis of migraine may be able to buy sumatriptan from a pharmacy, while other triptans are available on prescription.
The PJ survey also showed differing approaches to the use of triptans — 38% of pharmacists (n=69) said ‘when analgesia is ineffective’, and 32% (n=58) said ‘when analgesia and an antiemetic is ineffective’.
Killen suggested this difference may be owing to inconsistent national guidance around migraine management.
Inconsistent and out-of-date guidance may also be reflected in differing responses to the survey about preventative treatments for migraine. Most pharmacist respondents said they would recommend propranolol (81%; n=140), 70% said amitriptyline (n=121) and 59% said they would recommend candesartan (n=102).
Three-quarters said they would recommend topiramate (76%; n=132) — but this drug is now contraindicated in pregnancy and requires a Pregnancy Prevention Plan (PPP) to be in place, meaning it is likely to be inappropriate for use by most migraine patients who are female and of reproductive age.
The survey also found that 81% (n=140) of pharmacists — across all settings — were not familiar with migraine treatments that specifically target calcitonin gene-related peptides (gepants and CGRP monoclonal antibodies). More than half of pharmacists (53%; n=90) were unsure about whether patients in their area were finding it difficult to access newer treatments, while 16% (n=28) were aware of access issues.
When primary care clinicians make referrals to specialist care, these are often rejected as they do not include all the required information, such as recording that the patient had exhausted all other treatment options, Mathew Garrod, a specialist pharmacist in migraine at University Hospital Southampton NHS Foundation Trust, said.
With enablers, such as improved training and optimised care pathways in place and greater levels of pharmacist prescribing, there could be an opportunity for gepants and CGRP monoclonal antibodies to be initiated and managed in primary care.
Reviewing medication use and overuse
At the roundtable, Music suggested that migraine is “best managed in the primary care setting”.
Questionnaires may be a useful tool to help pharmacy teams understand a patient’s history and whether migraine is being well managed.
In addition to the WWHAM questions (who is the medication for, what are the symptoms, how long have you had the symptoms, what action has already been taken, are you taking any other medication?), roundtable attendees suggested using:
Pharmacists and pharmacy teams in both community and general practice should also encourage patients to keep a migraine diary, warn them about the risk of medicine overuse headaches, and support them with lifestyle advice to manage migraine.
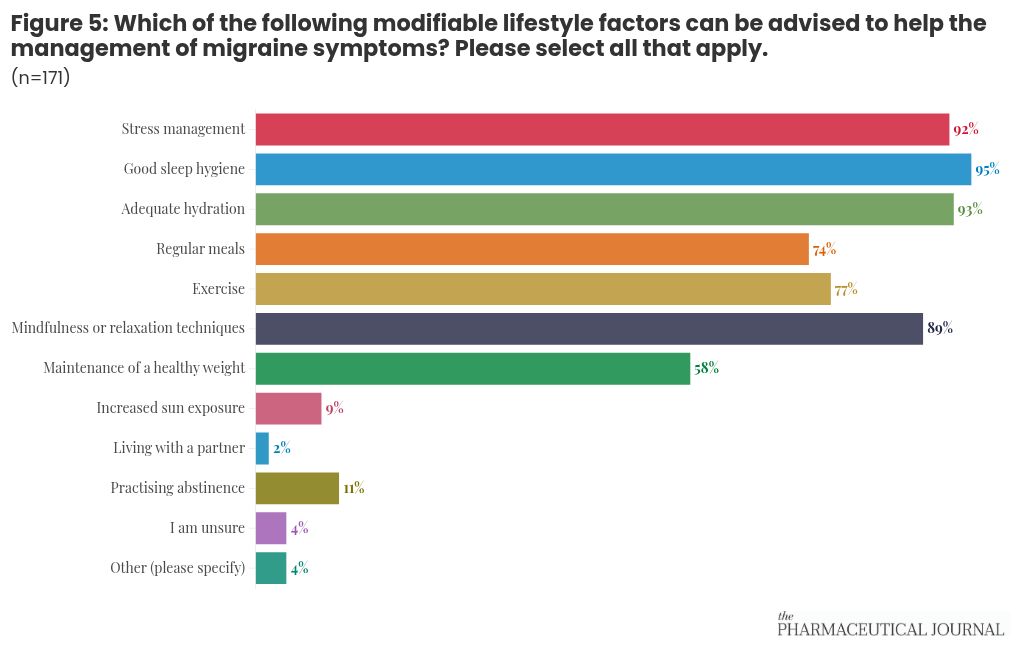
Responses to The PJ survey found that 53% (n=90) of pharmacists were ‘somewhat confident’ on providing lifestyle advice, while 29% (n=50) were confident or very confident. Pharmacists were able to correctly identify modifiable lifestyle factors, such as stress management, sleep hygiene, hydration, regular meals and exercise.
Regarding medicine overuse headaches, nearly two-thirds of primary care pharmacists (n=32) said they would counsel patients, while overall, 28% of respondents (n=48) said they ‘always’ did so and 20% (n=34) said they did so ‘rarely’ or ‘never’.
Laura Buckley, a primary care network pharmacist, suggested that patients with migraine could be identified from clinical systems, while advanced pharmacy technicians could be trained to use questionnaires to identify when a patient’s migraine is being well managed and when a patient may need further support.
Patients in need of more support could then be referred to a pharmacist for titration of medication and then, if necessary, the patient could be referred to specialist care, Buckley suggested.
Meanwhile, pharmacists working in primary care network (PCN) roles could ask patients about migraine during structured medication reviews (SMRs), as they do for other long-term conditions, she added.
“When I do SMRs, I like to cover as many conditions as the patient has. But how many patients are [we] asking: ‘How often are your migraines? What impact do they have on your daily life?’”
Buckley highlighted that once a patient was prescribed medication for migraine, either in secondary or primary care, “the expectation is that the patient will come back if it doesn’t work”.
However, she suggested that this needed to be communicated better with patients so that they were clear on what the next steps in their treatment should be, as the capacity for follow-up varies.
Learning from others
With financial support from the Scottish government, health board NHS Grampian has pioneered a comprehensive approach to migraine management, working with patients in their local area, to increase knowledge and confidence levels within community pharmacy.
The project included a live public education webinar, which was very well attended and improved understanding of migraine for nine in ten attendees.
Based on focus group feedback, the “number one enabler” for people accessing help for migraine through pharmacy “was knowing that pharmacists had the expertise to help them”, Katy Styles, clinical lead for realistic medicine at NHS Grampian, told the roundtable.
The project upskilled 50 community pharmacists in migraine management through an e-learning module and four live training events developed around Scotland’s national headache pathway. E-learning was found to be effective — the training was uploaded on to a single national healthcare learning platform and will continue to be updated by NHS Education for Scotland.
Meanwhile, in the East of England, a new regional strategy is being drafted that will include consideration of new ways of commissioning services and care pathways for neurological conditions, including migraine, recognising that sustainability and care closer to home relies on a different way of working.

Paul Stuart
Enablers for better migraine care in pharmacy
1. Guidance and pathways
In Scotland, a National Headache Pathway sets out a clear treatment pathway, including diagnosis, acute treatment and prophylaxis. Similar pathways have been developed in England and Wales but are not as well embedded in practice.
The PJ survey revealed that pharmacists often rely on out-of-date guidance, with 69% of pharmacist respondents (N=131) saying they would consult NICE guidance to diagnose and treat migraine — which did not include the latest treatments at the time.
The survey also found that 67% (n=127) of pharmacist respondents used the BNF, 52% used SmPc (n=98), and just 20% of pharmacists (n=37) used the British Association for the Study of Headache (BASH) guidelines. Only 7% of community pharmacists referred to BASH guidelines, compared with 28% in primary care, while 25% of community pharmacists said they do not refer to migraine guidelines at all.
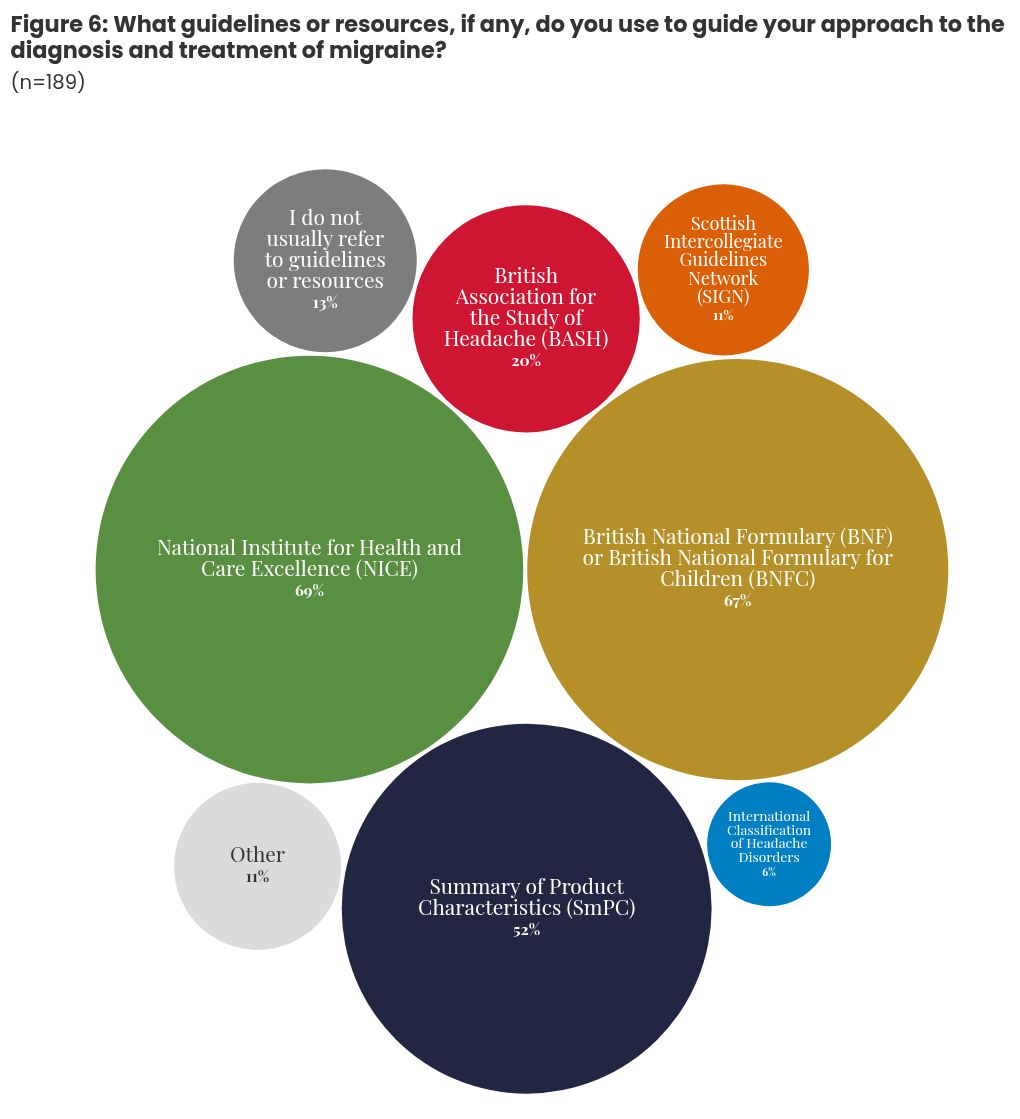
Munro noted that BASH guidance is in the process of being updated to include the newest treatments, with a rapid review due to conclude later in 2025.
Actions
- BASH and NICE guidance need to be updated [NB: see Box];
- Treatment pathways through primary, secondary and specialist care need to be made clear and embedded in practice.
2. Time and funding
Clinicians undertaking work around migraine often do so because of a personal interest in the condition — but it should become a “standard of care”, Duncan noted.
Pressures on all parts of the healthcare system may be a barrier to this but understanding the impact of migraine could help build a case for incentivising migraine care.
“Migraine [is] more common than diabetes, asthma and epilepsy combined,” noted Munro. And she said the Quality and Outcomes Framework (QOF) points attached to these conditions provided “an implicit motivation for GPs and practice staff” to work on them.
“There’s nothing like that for migraines. There’s no incentive,” Munro added.
Meanwhile, Buckley suggested that neighbourhood health funding might be used to support migraine services, such as peer support groups.
“There is funding that’s being allocated to primary care networks to allow us to do pieces of work locally, in supporting certain groups of patients that we feel within our locality they would benefit from,” Buckley said.
She shared that her PCN was considering using this funding to set up a group for patients with chronic pain, which could then be continued by patients themselves.
Buckley suggested that migraine support groups could be developed similarly, perhaps including guest speakers or sessions on lifestyle advice.
Juliana Ochulor, a nurse specialist at Guy’s & St Thomas’ NHS Foundation Trust, shared how the format had worked well with her patients, who take comfort and validation in connecting with others who understand the challenges of living with migraine.
“I did something very similar in a smaller group, whereby I always get all my patients for injections coming at two o’clock. They all have the same appointment time, I have a designated area with coffee, tea and biscuits. They all come in and chat to each other, befriend each other, talk about their condition… they feel empowered because they’re talking to people with similar conditions, and you, as a professional, you learn from it because you’re listening, you can see what their problem is, what medication they don’t like taking, why they don’t like taking it, what side effects they have. It’s a really good forum,” she said.
More broadly, the Migraine Trust is currently working on quantifying the health economic impact of migraine, and there may be opportunities for charities and pharmacy bodies to work together to educate the public about migraine management and how pharmacists and pharmacy teams can help.
Action
- Primary care networks should consider migraine as a focus area, and may be able to use neighbourhood health funding and other funding sources to deliver training, conduct migraine-focused SMRs, raise patient awareness and/or set up patient groups.

Paul Stuart
3. Training
A better understanding of migraine would help community and primary care pharmacy teams improve the advice and support they already offer as part of their day-to-day role, employing similar skills as they use for the management of other long-term conditions.
To enable this type of training, pharmacists need funded and protected learning time for training, rather than being expected to upskill in their own time, Buckley suggested.
Gareth Hughes, a superintendent community pharmacist in South Wales, suggested RPS and Health Education Wales funding for prescribers could be utilised to bring in a migraine specialist to deliver training for pharmacists.
As a pharmacy employer, he suggested that training delivered to pharmacists could then be passed on the rest of the team.
Roundtable attendees also called for more education about migraine at undergraduate level, especially with the opportunity for pharmacists to take on prescribing roles in migraine management and deliver care in the community, afforded by pharmacists joining the register as prescribers from 2026.
The survey found that 49% of pharmacists received one to five hours training on migraine in their undergraduate degree, while 47% received less than one hour (n=166). Based on responses from foundation trainees and students, the survey found that the amount of time being devoted to migraine training does not seem to have changed over time.
Attendees at the roundtable also highlighted that pharmacists should be aware of other conditions that often co-occur alongside migraine, such as mental ill-health — which may be caused by the lifestyle impact of migraine — as well as conditions with similar symptoms or which often co-occur with migraine, such as perimenopause, Ehlers-Danlos syndrome (EDS), postural orthostatic tachycardia syndrome (PoTS), hypermobility and neurodiversity.
Roundtable attendees also raised the importance of education for the wider pharmacy team, with pharmacy technicians being well-placed to assess patients for migraine symptoms and review whether current management is effective.
Actions
- Undergraduate pharmacist training should include an understanding of migraine, its impact and treatments, as well as comorbidities;
- Development of a pharmacist competency framework around headache and migraine, akin to those for nurses;
- Accredited education and training programme on migraine for pharmacists, their teams and pharmacies that is centrally hosted about migraine, building on and possibly incorporating those developed in NHS Grampian;
- Community pharmacy teams that have undertaken training on migraine could certify as a “migraine-friendly” pharmacy and display a badge that shows they are ready to support patients with migraine;
- The PJ and The Pharmacy Technician Journal could publish learning materials on the topic of migraine.
Conclusion
Overall, the roundtable highlighted the need for pharmacists and pharmacy teams, particularly in community pharmacy and primary care, to have a clear understanding of what migraine is, how it affects patients and the correct treatment pathway available. Education and training should be resourced and pharmacists and pharmacy team should ask the correct questions about migraine management when speaking to patients about their symptoms and treatment.
To build on the learnings from this event, The PJ will be developing a podcast episode, alongside identifying opportunities to continue the discussions and develop insight-led education and support materials.