Data sources
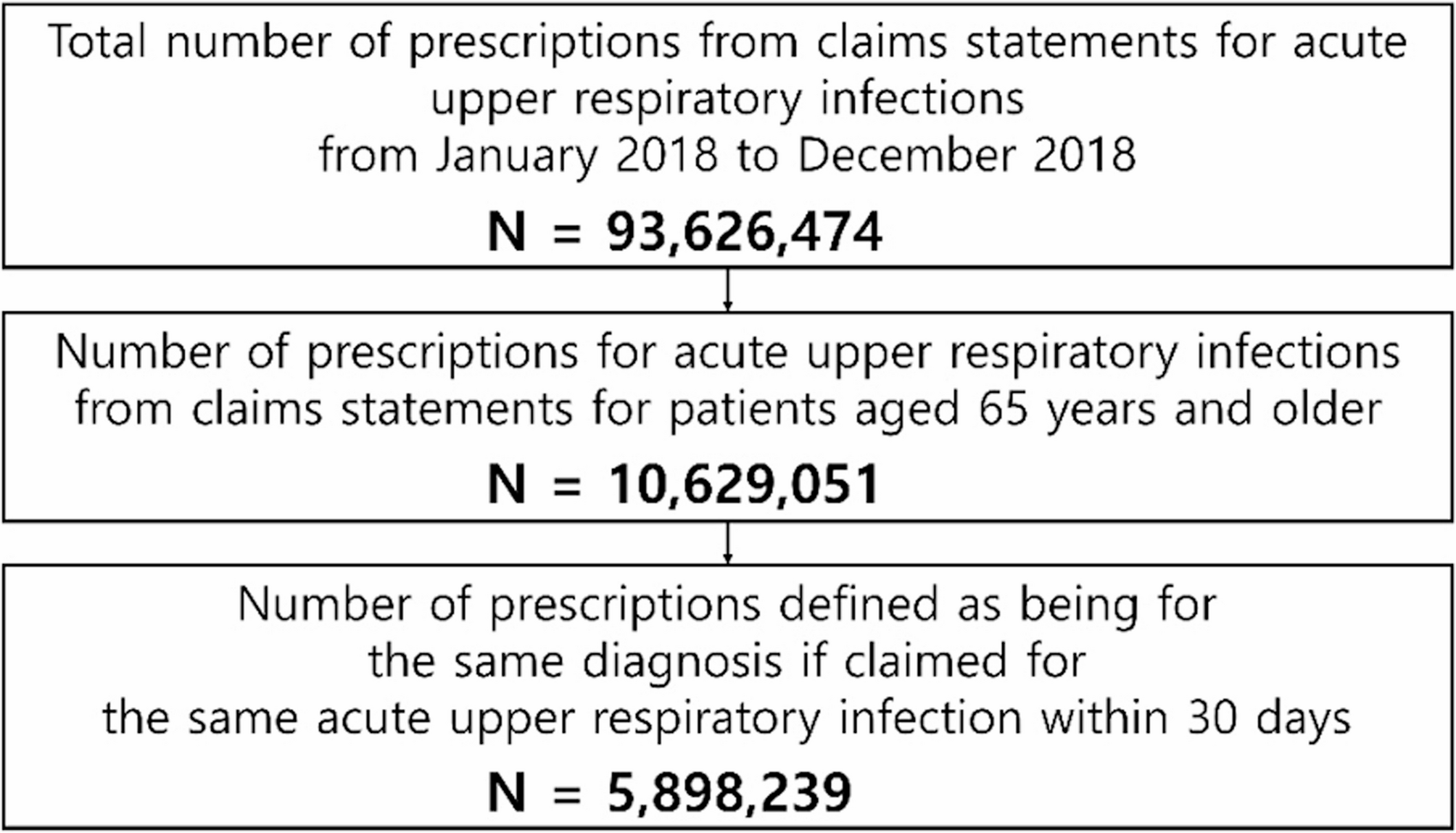
This retrospective study used National Health Insurance claims data collected by the Health Insurance Review and Assessment Service, a government agency responsible for reviewing healthcare services in the Republic of Korea. Data were collected from January 1, 2018 through December 31, 2018 to avoid confounding effects from the coronavirus disease 2019 pandemic. Of the 93,626,474 claims related to acute URIs, 10,629,051 claims were identified for those aged ≥ 65 years. Patients with multiple visits during a defined period were grouped as a single prescription unit; based on this criterion, we analyzed 5,898,239 prescription units (Fig. 1). The selected claims were categorized by the type of medical institution: primary, secondary, or tertiary.
Prescription categorization Prescriptions for individuals aged ≥ 65 years with an acute upper respiratory infection were extracted from claims statements
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the Korean Health Insurance Review and Assessment Service (protocol code: 2022-027-001, April 21, 2022).
Diagnostic categories
We selected diseases classified as acute URIs according to the International Classification of Diseases, 10th Revision (ICD-10). The analyzed conditions included acute nasopharyngitis (common cold) (J00), acute sinusitis (J01), acute pharyngitis (J02), acute tonsillitis (J03), acute laryngitis and tracheitis (J04), acute obstructive laryngitis and epiglottitis (J05), and acute upper respiratory infections of multiple and unspecified sites (J06). These were reported as the main diagnoses and the first through the fourth sub-diagnoses.
Prescription units
Each patient’s multiple healthcare visits for an acute URI were grouped into a single prescription unit, defined as a 30-day episode starting from the initial acute URI diagnosis date [9, 10]. All medical claims, diagnoses, and prescriptions occurring within this 30-day window were included as part of the same episode. Antibiotic prescription status was identified within each episode, and pneumonia diagnoses were assessed across the full study period of 2018. This approach allowed us to evaluate whether pneumonia was more commonly diagnosed during the year in patients who had received antibiotics during acute URI episodes, without assuming a temporal or causal sequence.
Variables of interest
The independent variables included sex, age, type of medical institution, and specialty. Age groups were categorized as 65–74, 75–84, 85–95, and > 95 years. The institutions were classified as primary, secondary, or tertiary. Specialties frequently associated with acute URIs included otolaryngology, internal medicine, general medicine, family medicine, and surgery; others were grouped as “other.”
We analyzed the prescription details for antibiotics and classified them as penicillin, cephalosporin (1st, 2nd, 3rd, or higher generation), macrolides, quinolones, and others, based on the Korean Health Insurance Review and Assessment Service drug benefit list and the Korea Food and Drug Administration classification.
Comorbidities were identified by ICD-10 codes for ischemic heart diseases (I20–I25), heart failure (I50), chronic obstructive pulmonary disease (COPD) (J43–J44, excluding J43.0), diabetes mellitus (E10–E14), and cancer (C00–C97), which are significant conditions often coexisting with pneumonia, and billed as the main and first four sub-diagnoses in the health insurance claim data.
Outcome variables
The primary outcome, pneumonia diagnosis, was identified from the 2018 claims, billed as the main and first four sub-diagnoses with specific disease codes: viral pneumonia (J12), pneumonia due to Streptococcus pneumoniae (J13), Haemophilus influenzae (J14), bacterial pneumonia (J15), pneumonia due to other organisms (J16), pneumonia in diseases classified elsewhere (J17), and unspecified organism (J18).
Statistical analyses
Descriptive statistics are used to describe the patient clinical characteristics. Chi-square and Fisher’s exact tests were used to assess the association between antibiotic prescription and pneumonia. Univariate logistic regression was used to identify factors associated with pneumonia diagnosis among patients with acute URIs. Multivariate logistic regression was then used to assess the association between antibiotic prescription and pneumonia diagnosis, with the results expressed as odds ratios (ORs) and 95% confidence intervals (CIs). Statistical significance was set at P < 0.05. Analyses were performed using SAS Enterprise Guide version 7.1 (SAS Institute Inc., Cary, NC, USA).