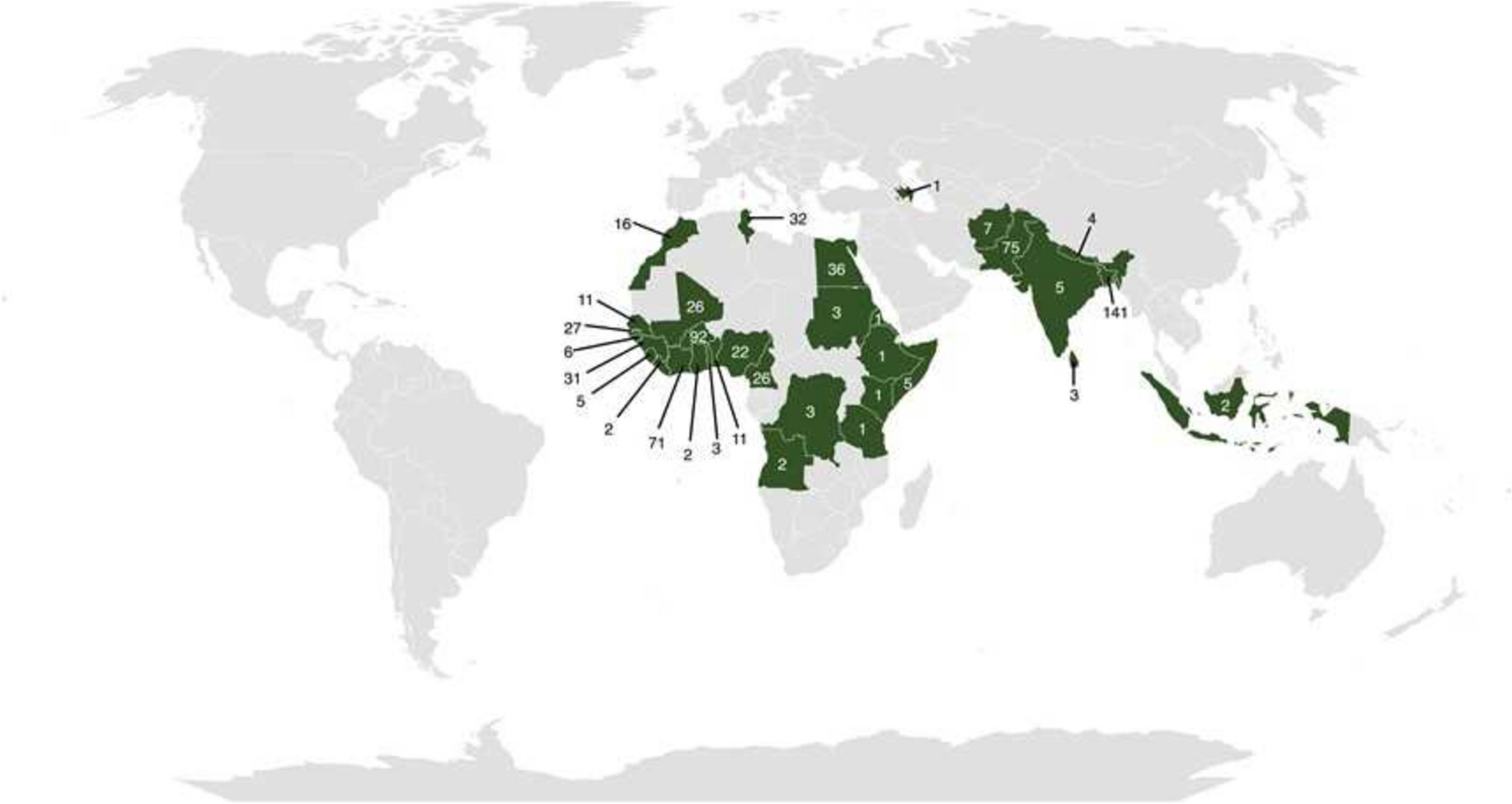
The first notable finding from our study is the significant shift in the geographical origin of migrants. The proportion of migrants from Asia has increased to 35.3%, compared to 21% in our previous study (p < 0.001) [8]. This shift aligns with global migration trends and the most recent Italian estimates [1, 2]. Such a change in the geographical origin of migrants should be considered when adapting guidelines and recommendations for screening both infectious and non-infectious diseases to the evolving epidemiological landscape.
In this context, our study offers an updated overview of the prevalence of infectious diseases among recently arrived migrants in Italy, nine years after our previous work in the same setting [8]. The findings further confirm the relevance of infectious diseases in this population, with significant differences observed based on migrants’ geographical origin.
HIV prevalence among migrants in this study was relatively low, with an overall rate of 1.5%, which is comparable to the prevalence observed in our previous study (1.3%) [8]. Similarly, there was a notable geographic disparity, with the majority of cases being observed among migrants from sub-Saharan Africa (90%). This is consistent with ECDC estimates as well as previous studies showing the highest HIV prevalence rates in sub-Saharan Africa, highlighting the continued need for comprehensive HIV screening and awareness programs targeting individuals from that geographical area [9, 10]. Although HIV prevalence was lower among migrants from Asia and North Africa in our cohort, we acknowledge that early diagnosis remains a public health priority. Therefore, our findings support the continued implementation of universal HIV screening among newly arrived migrants, irrespective of geographic origin.
Regarding HBV infection, 6.1% of participants were positive for HBsAg. Of note, HBsAg positivity in our study was lower than both our previous work (i.e. 11.6%) and similar studies on migrant populations [11]. Additionally, 55.1% of individuals had negative HBV serology, indicating a substantial proportion of susceptible individuals who could benefit from vaccination programs. The remaining 44.9% included both individuals with chronic HBV infection (6.1%) and those with serological evidence of past infection or immunity (i.e. anti-HBs and/or anti-HBc IgG positive, 38.8%). In particular, 75.9% of Asian migrants and 79.8% of North African migrants were eligible for HBV vaccination, emphasizing the need for tailored immunization strategies. Comparatively, the prevalence of chronic HBV infection (HBsAg positivity) in the general Italian population is approximately 0.8% [12]. The higher rate in our cohort, particularly among migrants from sub-Saharan Africa, likely reflects lower vaccination coverage and later adoption of universal vaccination in countries of origin. These findings support the importance of targeted screening and vaccination strategies aimed at newly arrived migrant populations to address health disparities.
Although the overall prevalence of HCV in our cohort was low (0.8%), it remains noteworthy, particularly among individuals from Pakistan. Only one of the five individuals with positive serology had detectable HCV-RNA, highlighting the importance of reflex testing for accurate diagnosis of active infection. This figure is comparable to or slightly lower than recent national estimates for the Italian general population, with anti-HCV antibody prevalence ranging around 1% and a viremic prevalence of approximately 0.66% [13]. These findings suggest that newly arrived migrants may not represent a significantly higher HCV burden compared to the host population; nonetheless, routine screening remains important to ensure early diagnosis and linkage to care.
Syphilis was detected in 2% of the migrants, which is consistent with findings from other studies that have addressed sexual health within migrant populations [14]. The prevalence was particularly high among sub-Saharan African migrants (3.5%) and relatively low in migrants from Asia and North Africa. In our previous study, 4.5% of participants from sub-Saharan Africa and 1.0% of those from Asia tested positive. This emphasizes the need for continued vigilance in screening for sexually transmitted infections, particularly in populations with higher rates of sexual risk behaviors and prior exposure in endemic regions.
Tuberculosis emerged as one of the most concerning findings in our study. The prevalence of TBI was 24.5%, while TB disease was diagnosed in 1.2% of participants, including both pulmonary and extrapulmonary forms. These results underscore the importance of comprehensive diagnostic strategies for TB among newly arrived migrants. The rate of TBI is consistent with epidemiological data from high-burden regions such as sub-Saharan Africa and Asia [15,16,17,18], from which most of our cohort originated. These findings reinforce the need to maintain systematic TB screening upon arrival in Europe and to initiate preventive treatment for TBI, which is essential to reduce the risk of disease reactivation and subsequent transmission within host countries.
A particularly relevant aspect of our study concerns helminthic infections. We observed an overall proportion of 12.3% for at least one helminthic infection diagnosed through a positive stool test and/or urine test, with clear differences by geographical region.
The prevalence of strongyloidiasis was 1.3%, which is consistent with the stool-based prevalence reported by Asundi et al. (1.8%) [19]. Our study also highlights a significant seroprevalence of strongyloidiasis (7.2%), with seropositivity markedly higher among Asian migrants (13.6%). Notably, our findings are lower than the pooled seroprevalence of 12.2% reported by Asundi et al. [19]. It should be noted that different serological assays have a wide range of sensitivity and specificity values, with most concerns relating the potential cross-reactivity with other nematodes [19, 20]. However, due to the potential development of severe or disseminated infection in cases of immunocompromise, treatment of individuals who are only positive for serology is considered justified. Therefore, in this setting, lower specificity is not regarded as problematic as lower sensitivity.
The prevalence of schistosomiasis was 12.9%, with all cases, as expected, found among migrants from sub-Saharan Africa. It is worth noting that our findings are higher than the stool-based prevalence of 0.95% and the urine-based prevalence of 6.8% reported by Asundi et al. [19]. Also, the seroprevalence for Schistosoma spp. in our cohort was higher (52.6%) than that reported by Asundi et al. (18.4%), likely reflecting the low specificity of the test and the need for alternative diagnostic approaches for schistosomiasis, similarly to strongyloidiasis [19].
Filariasis remains an underdiagnosed parasitic disease in migrant populations, with limited data available in non-endemic settings [21]. Data on the prevalence of filariasis among migrants in Europe remain scarce, and most available epidemiological evidence comes from studies conducted in endemic regions of Africa [22, 23]. This knowledge gap complicates the development of targeted screening strategies in migrant populations, particularly given the clinical implications of filarial infections. Loiasis has recently been associated with increased mortality in cases with a high microfilarial burden, with eyeworm and Calabar swellings as characteristic clinical features; however, the disease can also present with atypical, non-specific symptoms [24]. While infection with M. perstans is generally considered less severe than other filarial infections, it can still lead to long-term symptoms and complications in certain individuals, such as abdominal pain and dermatitis [25]. Moreover, the stool tests for other parasitic diseases, including hookworm and T. trichiura, revealed significant rates of infection, particularly among migrants from Asia.
These findings confirm that routine screening for helminths is key a component of migrant health assessments, especially since these infections are often asymptomatic in the early stages but can lead to severe health consequences if untreated [3, 4, 8]. The cost-effectiveness and ease of treatment for these parasitic infections further emphasize the importance of including them in national screening protocols for newly arrived migrants. Similar findings have been reported by the REDIVI network in Spain, which analyzed trends in imported infections among more than 14,000 migrants and travelers over the past decade, further supporting the value of structured screening approaches in Europe [26]. Moreover, the heterogeneity in infection prevalence by region of origin supports the need for geographically-tailored screening strategies. As migration patterns evolve over time, adopting a flexible, route- and country-based approach could improve the effectiveness and efficiency of screening programs. While our study did not formally propose such a framework, the data provided may contribute to its future development.
Eosinophilia was present in 18.3% of the screened migrants and was significantly associated with helminthic infections. This association was especially pronounced among migrants from sub-Saharan Africa and Asia. Our analysis confirmed that S. stercoralis and Schistosoma spp. were the most frequently associated parasites, in line with previous studies [27, 28]. Specifically, eosinophilia was observed in 18.2% of African migrants and 26.9% of Asian migrants, with the condition predominantly linked to schistosomiasis in African migrants and strongyloidiasis in Asian migrants. The sensitivity of eosinophilia as a marker for helminthiasis is well recognized, but its specificity remains low, as it can be influenced by non-infectious conditions such as allergies and autoimmune diseases [27, 29]. Remarkably, our findings suggest that eosinophilia alone is insufficient to rule out helminthic infections. Among S. stercoralis cases, 2/9 (22.2%) of infected individuals did not present eosinophilia, emphasizing the need for systematic screening. Similarly, 27/50 (54.0%) patients with Schistosoma spp. infections did not have eosinophilia, suggesting that chronic infections may not always trigger a sustained eosinophilic response [30]. These results highlight the importance of a combined diagnostic approach, integrating eosinophilia assessment with direct parasitological methods, serology, and molecular techniques to improve case detection.
One of the main limitations of our study is its retrospective nature, which may have affected the quality of data collection. A comparison of prevalence with data from previous studies is challenging due to differences in the definitions of helminthic infections and the use of various diagnostic tests for screening (e.g., different serological assays for S. stercoralis and Schistosoma spp.). Additionally, the collinearity between eosinophilia and the presence of certain parasites posed a challenge in constructing robust multivariable models to assess risk factors, as reflected in the wide confidence intervals of the OR estimates. An additional limitation is that eosinophilia was defined solely based on the absolute eosinophil count, without considering the eosinophil percentage. This approach may have entailed an underestimation of eosinophilia in individuals with low total leukocyte counts, such as those from sub-Saharan Africa. Furthermore, data on VDRL titers and previous syphilis treatment were inconsistently recorded and therefore could not be included in the analysis.
Furthermore, our findings reflect the specific characteristics of the local migrant population, which may limit their applicability to other settings with different demographic and epidemiological profiles. Additionally, the distinction between asylum seekers and undocumented migrants was not addressed in the paper, and no analysis was performed to explore potential differences between these two categories.
Finally, with regard to TB classification, we did not distinguish between subclinical and symptomatic forms of TB [31], as this distinction was beyond the scope and focus of the present study.