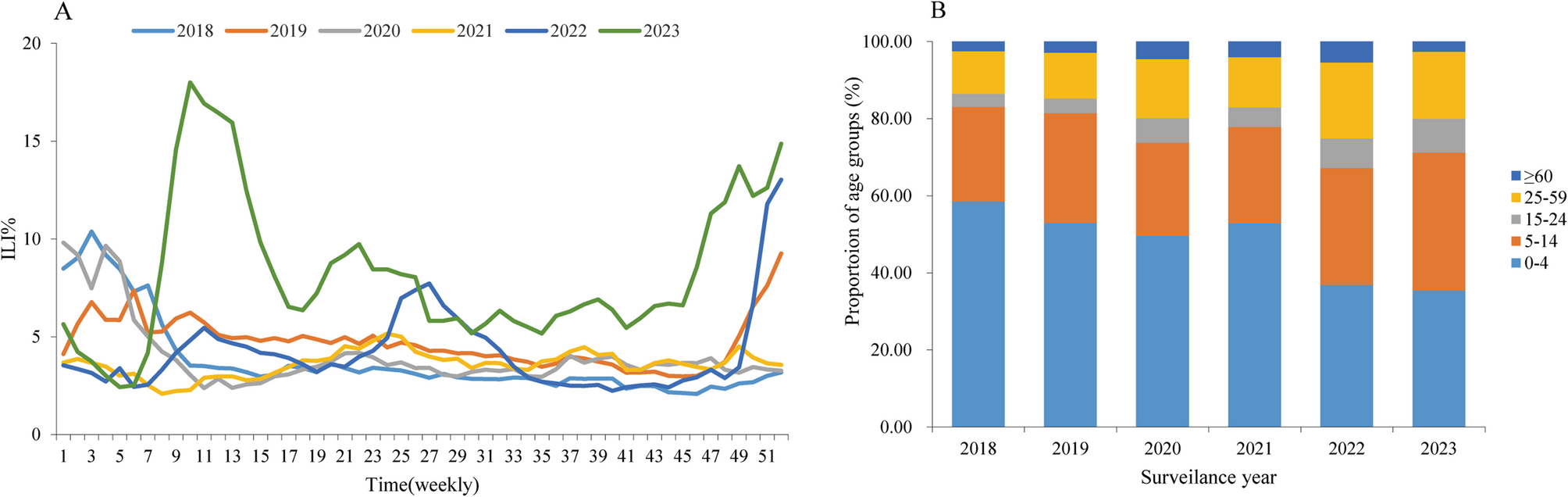
Influenza viruses are prone to mutation, necessitating long-term and systematic monitoring to identify their epidemic patterns and mutations promptly, and to inform the selection of vaccine strains and disease prevention and control strategies [13]. The results showed that both ILI% and the positive rate of influenza virus detection in Zhejiang Province in 2020 decreased significantly compared with that before the COVID-19 pandemic, remaining at a low epidemic level throughout the year without obvious seasonality, which was similar to the national influenza epidemic situation during the same period [14]. This may be attributed to the implementation of stringent nonpharmaceutical interventions (NPIs) against the COVID-19 in China from January 20, 2020, and the adoption of various public health prevention and control measures, which effectively prevented and controlled the COVID-19 outbreak and curtailed the spread of influenza [15, 16]. In 2021, the COVID-19 epidemic in China stabilized, and social production and life gradually returned, people’s awareness of prevention and control waned, leading to a resurgence in the influenza epidemic, with a peak in winter and spring. The influenza epidemic in 2022 featured three peaks in July, December, and March of the following year, with the positive rate of influenza virus nucleic acid detection similar to that of 2019 before the COVID-19 epidemic. The July peak may be related to factors such as the geographical location of Zhejiang Province [17]. Zhejiang Province is located in the southeast coastal area, during summer, it is often affected by typhoons and the rainy season, resulting in a decrease in temperature, which provides ideal conditions for the survival and spread of influenza viruses. Additionally, July is the summer vacation period in China, increased population mobility activities such as traveling and gatherings have accelerated the spread of influenza virus. ILI% showed a rapid upward trend from November 2022, peaking in December, but the positive detection rate of influenza virus during the same period was very low, suggesting that the rapid increase in ILI% maybe associated with the rapid and high-intensity spread of the COVID-19, and the majority of ILI patients were infected with SARS-CoV-2 [18]. Research findings reveal that in the context of the COVID-19 pandemic, influenza surveillance should integrate the consistency between ILI% and the positive detection rate of influenza virus, and simultaneously test for both influenza virus and SARS-CoV-2 in ILI and SARI samples to monitor the impact of COVID-19. In early 2023, the number of ILI cases in Zhejiang Province increased rapidly and peaked in March, primarily driven by A (H1N1) influenza viruses. This may be related to the easing of COVID-19-related NPIs of China on January 8, 2023, and the gradual resumption of social order and travel activities following the adjustment of various control measures. Additionally, the immunological gap related to the COVID-19 [19], the reduced immune function caused by SARS-CoV-2 [20, 21], and seasonal factors [22] are also important reasons for the post-COVID-19 influenza outbreak. Similar “triple outbreaks” of influenza, respiratory syncytial virus (RSV), and the COVID-19 have been observed in Europe and the United States since the release of the COVID-19 pandemic [23]. From a population distribution perspective, ILI cases in Zhejiang Province were predominantly concentrated in children under 5 years old, with fewer cases among the elderly. This is because children, due to their weaker immune systems, are a high-risk group for influenza infection and typically seek medical attention for symptoms such as fever and cough, whereas the elderly may seek treatment for other symptoms [24].
Etiological monitoring results showed that the positive rate of influenza virus varied across different years, with different dominant strains, exhibiting a general pattern of alternating A and B types. The primary reason may be that when a particular strain is circulating, the population gains some immunity, reducing the likelihood of reinfection with the same strain in subsequent years. Influenza virus positive rates were highest in children under 15 years old. Among younger populations, the proportions of influenza A and B were higher, while in older populations, the proportion of A (H3N2) was higher and the proportion of influenza B was lower. These findings are consistent with previous studies [25]. Notably, influenza B (Yamagata) cases were detected in 2018–2019 but were nearly absent during the COVID-19 pandemic, which was basically in line with the global epidemic trend of influenza B (Yamagata) [26]. This possibly related to the inherent vulnerability of this lineage. Indeed, the B (Yamagata) lineage has low antigenic diversity [27], lower effective reproduction number, and a shorter transmission chain compared with the B (Victoria) lineage [26], making non-pharmaceutical interventions more effective in controlling the B (Yamagata) lineage. Furthermore, the previously long-lived clades of B (Yamagata) went extinct maybe another reason for the decline of B (Yamagata) [28]. Lastly, in 2008–2019, the B (Yamagata) lineage demonstrated greater global movement than B (Victoria) lineage [28]. The B (Yamagata) lineage may have already been at a low prevalence cycle at the beginning of COVID-19 pandemic.
Influenza surveillance is conducted globally according to the ILI definition recommended by WHO. Theoretically, the positive rate of influenza virus nucleic acid detection should be positively correlated with the number of ILI cases. However, this study found that after the pandemic, the positive rate curve of influenza virus nucleic acid detection in the 0–4 years group did not align with the ILI curve, with more pronounced peaks and troughs. In particular, in 2020, after the implementation of strict prevention and control measures for the COVID-19 epidemic, the correlation between ILI number and the influenza virus positive rate has no significant difference in children under 15 years old, suggesting that children and infants often have multiple respiratory pathogen infections, the current definition of ILI may not be suitable for influenza surveillance in children.
After the COVID-19 pandemic, respiratory syncytial virus, adenovirus, mycoplasma pneumoniae, and other respiratory infectious diseases have superimposed in China [29], presenting new challenges for influenza prevention and control. Influenza vaccination remains the most effective means for preventing influenza, and efforts should be made to improve vaccination rates through optimized vaccination services and policy advocacy, particularly focusing on key groups such as healthcare workers, the elderly, young children, and individuals with chronic diseases. Public health authorities should enhance the dissemination of influenza prevention and control knowledge, timely issue influenza epidemic warnings and risk assessments, and raise public awareness of self-prevention and control. Emphasizing the mechanism of multi-disease prevention and control for respiratory infectious diseases and incorporating respiratory multi-pathogen surveillance into the influenza sentinel surveillance network is crucial for the precise prevention and control of influenza and other respiratory infectious diseases.
To ensure the quality and level of influenza network surveillance, the Zhejiang Provincial Center for Disease Control and Prevention annually evaluated the quality of influenza surveillance work of collaborating laboratories and sentinel hospitals in various cities every year. The evaluation mainly includes the completeness and timeliness of the monitoring data report, pathogen detection, specimen collection, and other related aspects. The influenza monitoring tasks in all cities were all completed satisfactorily. However, our study still has some limitations. First, we did not test for any pathogens other than influenza, which prevented us from ruling out other viral, bacterial, and fungal pathogens that could cause ILI. So, it is difficult to determine whether the number of ILI cases is caused by SARS-CoV-2. Second, due to the unavailability of influenza vaccination rates across years and age groups of Zhejiang province, leading us unable to conform the exact impact of the COVID-19 pandemic on influenza.