Study setting
This study was conducted at four major healthcare facilities in Northwest Ethiopia including Debre Markos Comprehensive Specialized Hospital, Tibebe Gihon Comprehensive Specialized Hospital, University of Gondar Comprehensive Specialized Hospital, and Felege Hiwot Comprehensive Specialized Hospital.
Study period and design
The study was conducted, from January 1, 2023, to May 31, 2023. A retrospective cohort design was employed to assess existing medical records, using a one year dataset.
Source and study population
The study population consisted of patients diagnosed with comorbid mental health and cardiovascular diseases who received care at the participating hospitals. Patients were identified through hospital admission and discharge records, outpatient clinic logs, and electronic health records.
Eligibility criteria
The inclusion criteria for participants were:
-
A confirmed diagnosis of comorbid mental health and cardiovascular disease in medical records.
-
Age 18 years or older at the time of diagnosis.
-
Available medical records for the duration of the study period.
The exclusion criteria for participants were:
-
Patients with incomplete medical records,
-
Those who had prior cardiovascular surgeries.
-
Individuals with terminal illnesses unrelated to comorbid mental health and cardiovascular diseases.
Study variables
The dependent variables are hospital readmission and emergency department visits. The independent variables included mental health treatment, age, sex, and residence.
Sample size determination
This study included all patients who met the eligibility criteria during the study period. As the study design was based on medical record review, no a priori sample size or power calculation was performed. Instead, the full population of eligible patients included to maximize statistical power and ensure generalizability.
A total of 319 patients with comorbid mental health and cardiovascular diseases between January 2018 and December 2022 were identified from four healthcare institutions in Northwest Ethiopia. These institutions were selected in simple random approaching method.
Sampling technique
To ensure the sample was representative of the eligible population across the participating hospitals, a proportional simple random sampling technique was employed. The total number of eligible patients at each hospital during the study period was first identified through a manual review of patient records. Proportional allocation was then used to determine the number of patients to include from each hospital based on its share of the total eligible patient population.
The formula used for proportional allocation was: ni = (Ni / N) × n.
Where:
-
ni = sample size from hospital i.
-
Ni = number of eligible patients in hospital i.
-
N = total number of eligible patients across all hospitals.
-
n = total sample size (319).
Based on estimated eligible patient numbers from hospital records (N = 1,100), the sample was allocated as follows:
-
Debre Markos Comprehensive Specialized Hospital: n1 = (360 / 1100) × 319 ≈ 104 patients.
-
University of Gondar Comprehensive Specialized Hospital: n2 = (300 / 1100) × 319 ≈ 87 patients.
-
Felege Hiwot Comprehensive Specialized Hospital: n3 = (240 / 1100) × 319 ≈ 70 patients.
-
Tibebe Gihon Comprehensive Specialized Hospital: n4 = (200 / 1100) × 319 ≈ 58 patients.
After determining the number of participants per hospital, simple random sampling was applied within each hospital. Eligible patient lists were prepared, and random numbers were generated using a computer-based random number generator to select participants independently.
Data collection procedure
This study employed a structured questionnaire, developed after an extensive review of relevant literature. The data collection instrument designed to capture sociodemographic characteristics, clinical parameters, and medication-related variables, with all data extracted from patient medical records. Comorbid conditions including diabetes mellitus, hyperlipidemia, hypertension, and other chronic physical conditions were identified based on clinician-documented diagnoses in the medical charts. Comorbidity was considered present if it was recorded in the patient’s medical history, diagnostic summary, or treatment plan during admission or follow-up visits. These conditions were categorized as binary variables (present or absent), and no additional thresholds related to disease severity, duration, or laboratory values were applied due to variability in documentation across sites.
Multiple methodologies were employed to assess the receipt of mental health treatment. Pharmacy refill records were used to determine whether patients actively received prescribed mental health medications during the study period. The duration of these prescriptions was also assessed as a measure of adherence to treatment regimens. Patient charts were systematically examined for indications of mental health treatment, including therapist notes, treatment plans, and mental health evaluations. Specific diagnosis codes associated with mental health conditions were identified to establish a clear connection between diagnosis and treatment. In addition to assessing the receipt of treatment, clinical outcomes related to mental health treatment were analyzed. Indicators such as psychiatric symptoms, changes in diagnoses, and hospitalization rates for mental health crises were assessed. To examine emergency department visits, patient medical records were reviewed throughout the study period. Details such as the reason for each visit, clinical diagnoses, and related mental health assessments were recorded. Visits were categorized based on their connection to comorbid mental health and cardiovascular diseases, mental health crises, or other health complications. For hospital readmissions, a similar review of patient medical records was conducted to track subsequent admissions within a specified follow-up period after discharge. Diagnosis dates were extracted from electronic health records, inpatient and outpatient medical charts, and physician notes. Diagnosis dates were extracted from electronic health records, inpatient and outpatient medical charts, and physician notes. For psychiatric disorders, clinical evaluations, mental health treatment initiation records, and International Classification of Diseases (ICD-10) codes were reviewed, with specific codes. For cardiovascular conditions, diagnostic imaging reports, laboratory results, and physician-confirmed diagnoses, along with corresponding ICD-10 codes, were examined. When exact diagnosis dates were unavailable, the earliest documented evidence of the condition, based on clinical evaluations or treatment initiation was recorded. Given the study’s focus on comorbid mental health and cardiovascular diseases, special attention was given to cases where the timing of psychiatric and cardiovascular diagnoses differed. For patients with pre-existing psychiatric disorders, the timing of the CVD diagnosis was recorded as the key event indicating the onset of a comorbid mental health and cardiovascular diseases. Conversely, for patients with pre-existing CVD, the timing of the psychiatric disorder diagnosis was recorded as the key event. In instances where both conditions were diagnosed simultaneously (e.g., during a single hospital admission), this date was recorded as the timing for both conditions. For patients with multiple episodes of the same condition, such as recurrent depressive episodes or repeated cardiovascular events, the first documented diagnosis within the study period was used.
Operational definitions
-
Comorbid mental health and cardiovascular diseases are health conditions that involve both cardiovascular disorders and psychiatric disorders.
-
Mental health treatment refers to interventions aimed at alleviating symptoms and improving the well-being of patients with diagnosed mental health conditions.
-
Hospital readmission is defined as any unplanned admission to the hospital. In this study, readmissions included those which are related to comorbid mental health and cardiovascular diseases.
-
Emergency department visit is any encounter in the emergency department requiring immediate medical attention. In this study, emergency department visits included those related to comorbid mental health and cardiovascular diseases.
-
Event Occurred: refers patients who experienced the outcome of interest during the study period, including those who had a hospital readmission or an emergency department visit.
-
Censored: refers patients who did not experience the outcome of interest (hospital readmission or emergency department visit) during the follow-up period. These individuals remained under observation but did not have the event occur before the study’s conclusion or were lost to follow-up.
-
Survival time (time to event): This is the duration from the start to the event.
Data quality assurance
To ensure the integrity and reliability of the data collected in this study, several quality assurance measures were implemented throughout the data collection process. A structured questionnaire was initially developed based on a comprehensive review of relevant literature, to facilitate standardized data capture across all participating institutions. The questionnaire was pre-tested on a small sample of medical records to identify ambiguities, improve clarity, and refine variable definitions prior to full-scale implementation.
Trained research assistants, all of whom were clinical pharmacists, conducted the data extraction. These data collectors underwent rigorous training on the study protocol, ethical considerations, operational definitions, and standard procedures for interpreting medical records. To assess and enhance inter-rater reliability, a pilot exercise was conducted in which 10% of patient charts were independently reviewed by two data collectors. Discrepancies were discussed and resolved through consensus, leading to adjustments in the protocol where necessary. Throughout the data collection period, Periodic supervisory audits were performed. The principal investigator and hospital-based site coordinators randomly reviewed approximately 10% of extracted data to verify accuracy and adherence to protocol. Any inconsistencies were addressed through targeted feedback and retraining sessions with the data collectors. Throughout the study period to ensure compliance with data collection protocols and to address any potential issues promptly. To minimize information bias, diagnoses were confirmed using multiple sources of documentation. Psychiatric disorders were validated by cross-referencing ICD-10 codes with therapist notes, treatment plans, and prescription records. Cardiovascular diagnoses were corroborated using physician-confirmed diagnoses, laboratory and imaging reports, and treatment documentation. In cases where exact diagnosis dates were missing, the earliest documented clinical evidence such as first mention of symptoms or treatment initiation was used as a proxy. To reduce the impact of missing data, records lacking essential variables (e.g., confirmed diagnoses or outcome data) were excluded from analysis. For less critical variables, a complete-case analysis was performed. Given the low frequency of missing data in those variables, imputation methods were not necessary. When feasible, missing details were recovered through triangulation across multiple record sources. To mitigate selection bias, a total population sampling strategy was used. All eligible patients with coexisting psychiatric and cardiovascular conditions who met the inclusion criteria and received care at any of the four participating hospitals were included. Additionally, all medical records and documentation were verified against the entries in the database to confirm accuracy and completeness.
Data processing and analysis
Data processing and analysis for this study were conducted using statistical software to ensure accurate interpretation of the findings. Following data collection, all questionnaires and medical record entries were reviewed for completeness and consistency. The data were then coded and entered into a secure electronic database to facilitate analysis. Descriptive statistics were generated to summarize the demographic and clinical characteristics of the study population. Categorical variables were described using frequency distributions and percentages, while continuous variables were summarized using means and standard deviations.
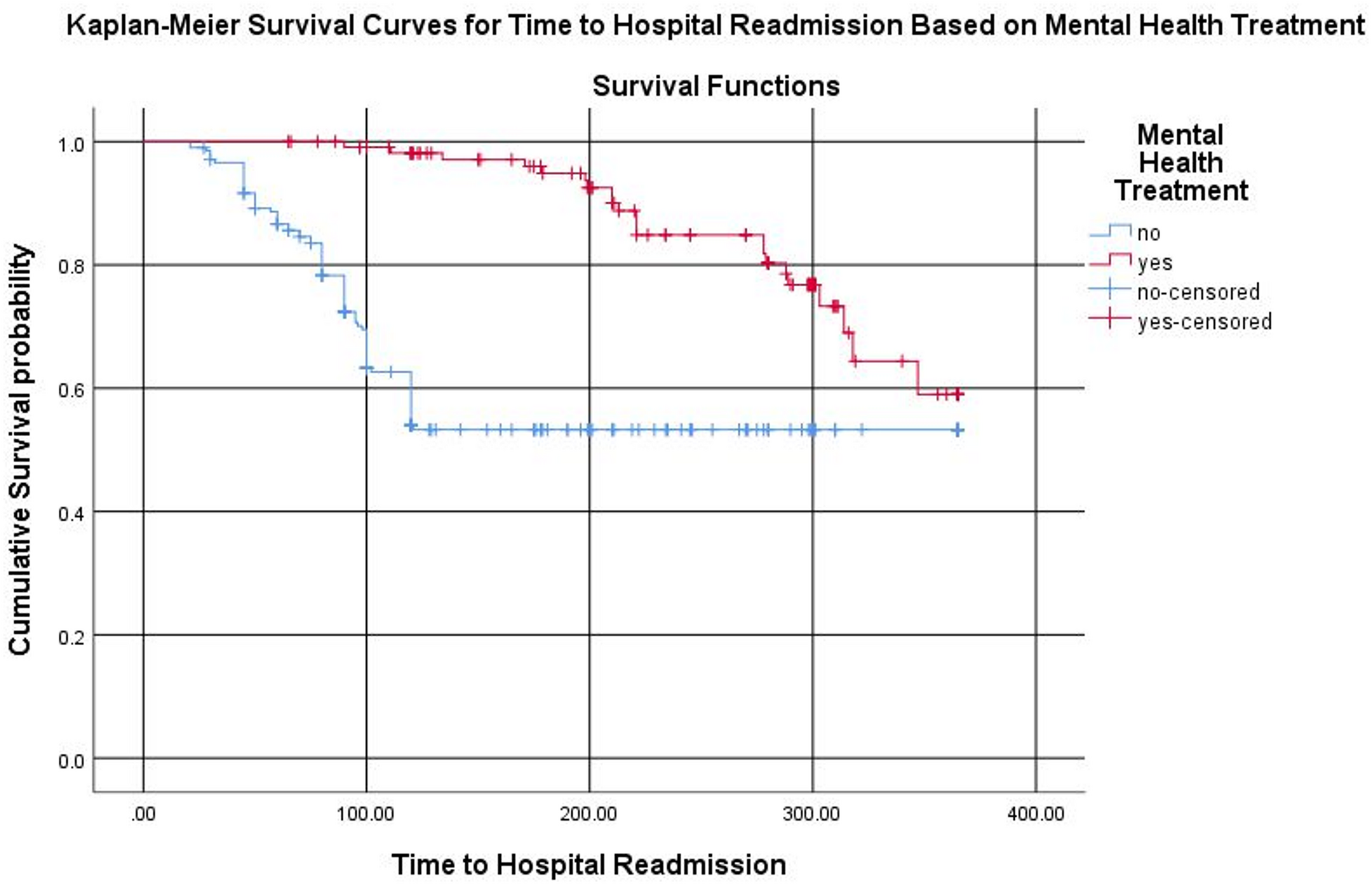
To identify factors influencing survival outcomes, Cox proportional hazards regression analysis was performed. The primary outcomes were the time to hospital readmission and the time to the first emergency department visit, both measured in days from the date of discharge or study entry. The follow-up period spanned one year from the date of the first diagnosis or discharge, with censoring applied at the end of the study period or upon loss to follow-up. The assumptions of the Cox proportional hazards model were evaluated using the Schoenfeld residual test. To examine the relationship between baseline variables and patient survival, a two-step approach was employed. Initially, each baseline variable that satisfied the assumptions of the Cox proportional hazards model was analyzed individually using separate Cox regression models. Subsequently, variables with a P-value of less than 0.25 in the bivariate analysis were included in the multivariable analysis. However, final inclusion was not based solely on statistical criteria. We also incorporated variables based on their clinical relevance, biological plausibility, and established evidence from prior studies on mental health and cardiovascular outcomes. The Cox regression model was utilized to identify factors associated with the time to hospital readmission and emergency department visit. The results were reported as crude hazard ratios (CHR) and adjusted hazard ratios (AHR) with corresponding 95% confidence intervals, and statistical significance was determined at a P-value threshold of < 0.05. Additionally, multicollinearity among the independent variables was assessed using the variance inflation factor to detect and eliminate redundant variables that could bias the estimates. The overall mean VIF was calculated to be 1.21, which falls within the acceptable range of 1 to 5. Survival analysis was further conducted using Kaplan-Meier survival curves to illustrate survival functions, and the log-rank test was applied to compare survival distributions between patients who received mental health treatment and those who did not.