The major findings of this review were: 1) Adding HRV and HRC to existing trauma triage scores or vital signs such as heart rate in pre-hospital patients could increase ability to distinguish between patients subsequently received an LSI. 2) Adding HRV and HRC to traditional triage scores could potentially be incorporated using existing hardware. 3) Over time there has become less ECG noise which increases quality of ECG data from four studies.
The patients in the included articles were respectively transported to hospitals in US, Singapore, Brussels. To insure a reliable and representative cohort of included patients, the cohorts were compared to a large study conducted in UK and Germany. This study included 68.510 patients, whereas the mean age was 56.3 ± 22.7, 65.7% of the patients were male [16]. These numbers match with the demography of the patients in the included articles.
Traditional vital signs were not all always useful predictors for a subsequent LSI even though HR to a certain extent were related to LSI [4, 15]. One of the most utilized vital signs included in triage scores is blood pressure, but in the studies included in this review, blood pressure measurement was not found as a predictor for LSI’s. An explanation for this could be the autonomic sympathetic drive compensating found in otherwise healthy persons when experiencing e.g. hemorrhage. The increased sympathetic drive compensating for blood loss could hypothetically be measured as a decrease in HRV and/or HRC. This decrease in HRV and/or HRC could potentially help to identify patients with normal vital signs otherwise getting overlooked as stable, but who subsequently will receive an LSI [12].
Even though no correlations were found between patients who received an LSI and those who did not with normal vital signs, the ∆AUC was 0.10 when adding HRV to the existing trauma triage score comprising vital signs and GCS. This agrees with the included studies, finding heart rate metrics from ECGs beneficial for discriminating between patients who subsequently will receive an LSI and who will not.
The integration of heart rate variability metrics into pre-hospital trauma triage remains unestablished, and a potentially attributing factor for this could be challenges posed by ECG analysis noise. This noninvasive vital parameter is derived from cutaneous electrical leads which cause increased ectopy and artifacts on the ECG, especially in a remote setting or en-route transport. This instigates ineligible ECG waveforms [4], has been noticeable in previous studies, where between 34 to 74% of ECG records were excluded due to noise [12, 13]. Good ECG recording with limited noise is therefore essential before implementing HRV/HRC as a triage parameter. The studies with high share of noise are respectively from 2008 and 2010, whereas a newer article from 2016 established that registration of in-hospital HRV is both feasible and reliable, with an exclusion rate of only 0.6% of the patients due to ECG noise [10] (Table 3). This could indicate that noise reduction and better ECG recording is already developed, which decreases noise on ECG and its influence on analysis.
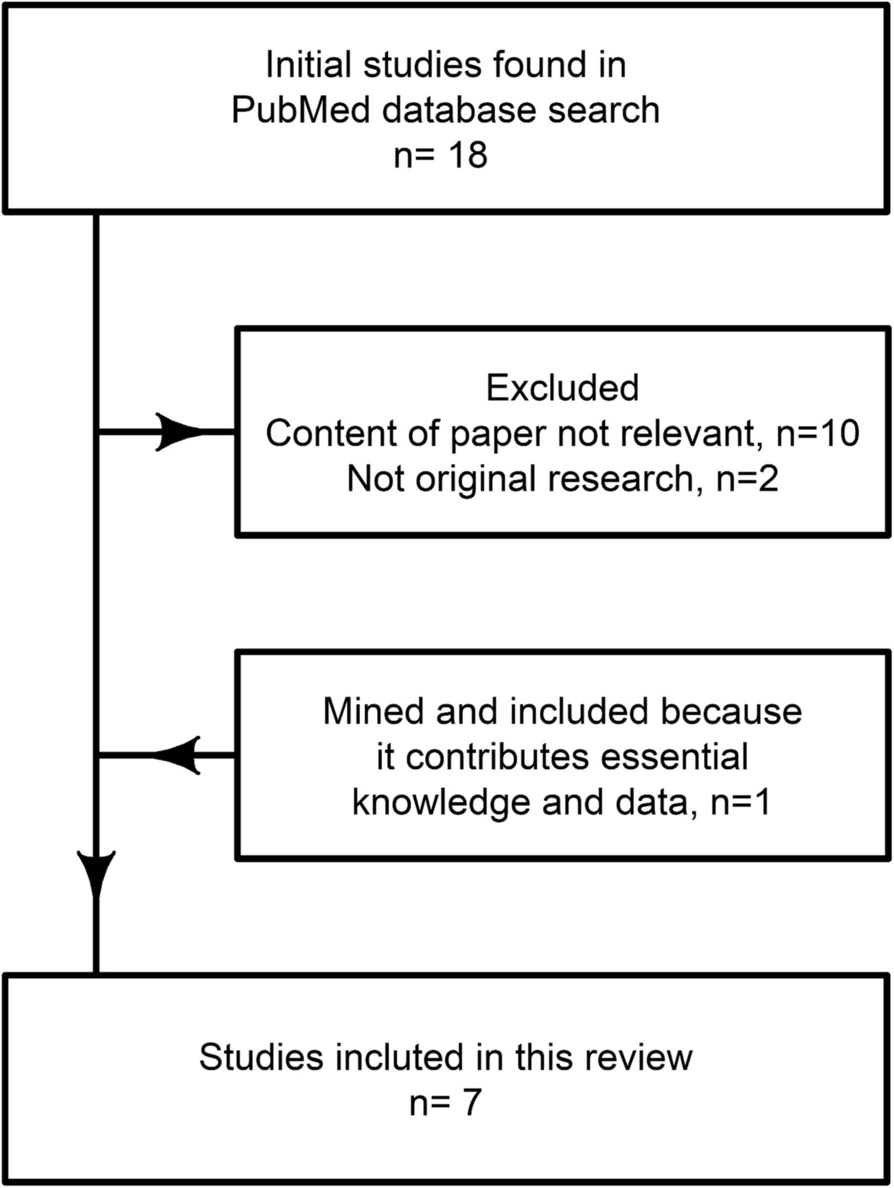
Other limitations include interindividual variability, chronic diseases and comorbidities e.g. ischemic heart disease and diabetes which has shown to affect HRV and HRC a great deal, but this data was not available in the included studies, hence these must be regarded as unmeasured confounders [5, 12]. The number of patients examined in the included studies ranges from 55 to 374 (Table 1). Larger studies could potentially increase robustness and include a greater variety of comorbidities in the study cohort, hence a more diverse population of patients. This could potentially identify sub-groups were HRV and HRC is more or less useful in triage.
In all the studies included, an analysis of ECG waveforms showed great/high predictive value for triage of pre-hospital patients. The results show an even greater/higher ∆AUC when incorporating this heart rate analysis in ROC. This is supported by the notion that one of the studies found no significant correlation while using HRV but did with HRC. This suggests that this more complex heart rate analysis techniques could achieve even higher predictive value than HRV. This would not pose a limitation, as the ECG metrics remain consistent regardless of the techniques employed.
In the studies included HRV and/or HRC was added to existing triage scores which gives credence to the notion of incorporating the two heart rate variability metrics to the traditional vital signs and not as independent triage scores to distinguish patients who will be needing LSI from patients who will not [5, 12].
A variation of analysis techniques was applied to the ECG metrics to derive HRV and HRC in the studies. The technique showing the greatest independent AUC was SampEn (0,76). SampEn and ApEn are similar analysis techniques computationally, but they still vary a bit and both of them have been included in multiple of the papers. SampEn displays more suitable characteristics for pre-hospital triage hence a decrease in the amount of QRS complexes has relatively little effect on it. SampEn can function with a data set down to approximately 100 beats [13]. While other techniques usually need up to 800 consecutive beats [12].
As aforementioned two studies found high negative predictive values and low positive predictive values. This means that potentially healthy patients were over-triaged. This can turn out to be more costly due to the larger number of patients needing rapid evacuation and the need for LSI according to HRV/HRC. But on the other hand, with a large negative predictive value less patients will be triaged as non-LSI when they need medical interventions.